
UPMC Health Benefits: Dental Schedule of Benefits 2025
An overview of dental benefits coverage, including deductibles and co-payments for participating and non-participating dentists under the UPMC Health Plan in 2025.
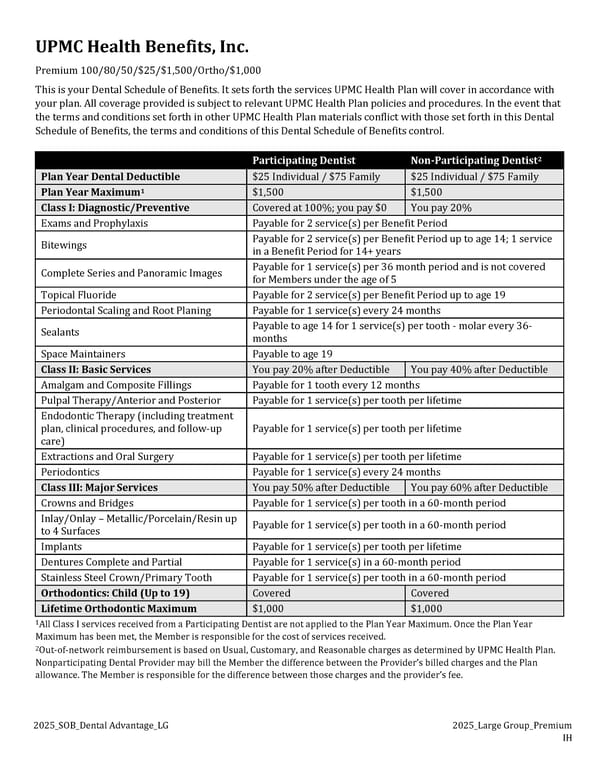
2025_SOB_Dental Advantage_LG 2025_Large Group_Premium IH UPMC Health Benefits, Inc. Premium 100/80/50/$25/$1,500/Ortho/$1,000 This is your Dental Schedule of Benefits. It sets forth the services UPMC Health Plan will cover in accordance with your plan. All coverage provided is subject to relevant UPMC Health Plan policies and procedures. In the event that the terms and conditions set forth in other UPMC Health Plan materials conflict with those set forth in this Dental Schedule of Benefits, the terms and conditions of this Dental Schedule of Benefits control. Participating Dentist Non-Participating Dentist2 Plan Year Dental Deductible $25 Individual / $75 Family $25 Individual / $75 Family Plan Year Maximum1 $1,500 $1,500 Class I: Diagnostic/Preventive Covered at 100%; you pay $0 You pay 20% Exams and Prophylaxis Payable for 2 service(s) per Benefit Period Bitewings Payable for 2 service(s) per Benefit Period up to age 14; 1 service in a Benefit Period for 14+ years Complete Series and Panoramic Images Payable for 1 service(s) per 36 month period and is not covered for Members under the age of 5 Topical Fluoride Payable for 2 service(s) per Benefit Period up to age 19 Periodontal Scaling and Root Planing Payable for 1 service(s) every 24 months Sealants Payable to age 14 for 1 service(s) per tooth - molar every 36- months Space Maintainers Payable to age 19 Class II: Basic Services You pay 20% after Deductible You pay 40% after Deductible Amalgam and Composite Fillings Payable for 1 tooth every 12 months Pulpal Therapy/Anterior and Posterior Payable for 1 service(s) per tooth per lifetime Endodontic Therapy (including treatment plan, clinical procedures, and follow-up care) Payable for 1 service(s) per tooth per lifetime Extractions and Oral Surgery Payable for 1 service(s) per tooth per lifetime Periodontics Payable for 1 service(s) every 24 months Class III: Major Services You pay 50% after Deductible You pay 60% after Deductible Crowns and Bridges Payable for 1 service(s) per tooth in a 60-month period Inlay/Onlay – Metallic/Porcelain/Resin up to 4 Surfaces Payable for 1 service(s) per tooth in a 60-month period Implants Payable for 1 service(s) per tooth per lifetime Dentures Complete and Partial Payable for 1 service(s) in a 60-month period Stainless Steel Crown/Primary Tooth Payable for 1 service(s) per tooth in a 60-month period Orthodontics: Child (Up to 19) Covered Covered Lifetime Orthodontic Maximum $1,000 $1,000 1All Class I services received from a Participating Dentist are not applied to the Plan Year Maximum. Once the Plan Year Maximum has been met, the Member is responsible for the cost of services received. 2Out-of-network reimbursement is based on Usual, Customary, and Reasonable charges as determined by UPMC Health Plan. Nonparticipating Dental Provider may bill the Member the difference between the Provider’s billed charges and the Plan allowance. The Member is responsible for the difference between those charges and the provider’s fee.
 UPMC Health Benefits: Dental Schedule of Benefits 2025 Page 2
UPMC Health Benefits: Dental Schedule of Benefits 2025 Page 2