
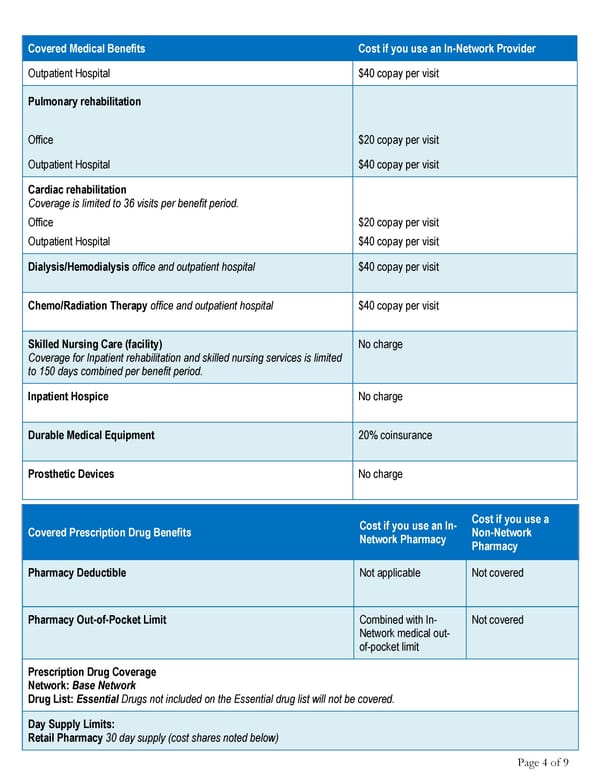
Covered Medical Benefits Cost if you use an In-Network Provider Outpatient Hospital $40 copay per visit Pulmonary rehabilitation Office $20 copay per visit Outpatient Hospital $40 copay per visit Cardiac rehabilitation Coverage is limited to 36 visits per benefit period. Office $20 copay per visit Outpatient Hospital $40 copay per visit Dialysis/Hemodialysis office and outpatient hospital $40 copay per visit Chemo/Radiation Therapy office and outpatient hospital $40 copay per visit Skilled Nursing Care (facility) No charge Coverage for Inpatient rehabilitation and skilled nursing services is limited to 150 days combined per benefit period. Inpatient Hospice No charge Durable Medical Equipment 20% coinsurance Prosthetic Devices No charge Cost if you use an In- Cost if you use a Covered Prescription Drug Benefits Network Pharmacy Non-Network Pharmacy Pharmacy Deductible Not applicable Not covered Pharmacy Out-of-Pocket Limit Combined with In- Not covered Network medical out- of-pocket limit Prescription Drug Coverage Network: Base Network Drug List: Essential Drugs not included on the Essential drug list will not be covered. Day Supply Limits: Retail Pharmacy 30 day supply (cost shares noted below) Page 4 of 9
 Anthem Classic HMO 20/40/500 admit/250 OP Summary Page 3 Page 5
Anthem Classic HMO 20/40/500 admit/250 OP Summary Page 3 Page 5