
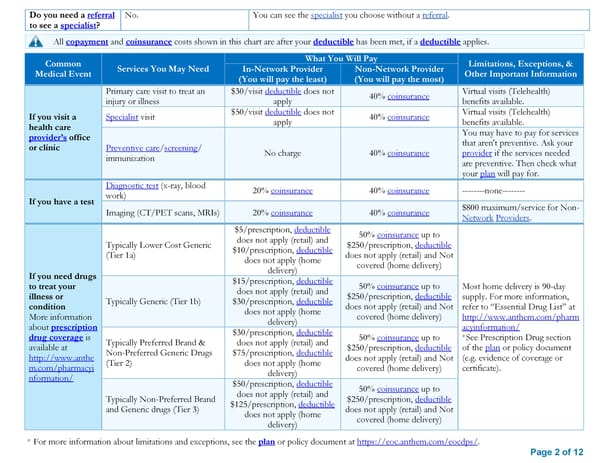
Do you need a referral No. You can see the specialist you choose without a referral. to see a specialist? All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common What You Will Pay Limitations, Exceptions, & Medical Event Services You May Need In-Network Provider Non-Network Provider Other Important Information (You will pay the least) (You will pay the most) Primary care visit to treat an $30/visit deductible does not 40% coinsurance Virtual visits (Telehealth) injury or illness apply benefits available. If you visit a Specialist visit $50/visit deductible does not 40% coinsurance Virtual visits (Telehealth) health care apply benefits available. provider’s office You may have to pay for services or clinic Preventive care/screening/ that aren't preventive. Ask your immunization No charge 40% coinsurance provider if the services needed are preventive. Then check what your plan will pay for. Diagnostic test (x-ray, blood 20% coinsurance 40% coinsurance --------none-------- If you have a test work) Imaging (CT/PET scans, MRIs) 20% coinsurance 40% coinsurance $800 maximum/service for Non- Network Providers. $5/prescription, deductible 50% coinsurance up to Typically Lower Cost Generic does not apply (retail) and $250/prescription, deductible (Tier 1a) $10/prescription, deductible does not apply (retail) and Not does not apply (home covered (home delivery) If you need drugs delivery) to treat your $15/prescription, deductible 50% coinsurance up to Most home delivery is 90-day illness or does not apply (retail) and $250/prescription, deductible supply. For more information, condition Typically Generic (Tier 1b) $30/prescription, deductible does not apply (retail) and Not refer to “Essential Drug List” at More information does not apply (home covered (home delivery) http://www.anthem.com/pharm about prescription delivery) acyinformation/ drug coverage is $30/prescription, deductible 50% coinsurance up to *See Prescription Drug section available at Typically Preferred Brand & does not apply (retail) and $250/prescription, deductible of the plan or policy document http://www.anthe Non-Preferred Generic Drugs $75/prescription, deductible does not apply (retail) and Not (e.g. evidence of coverage or m.com/pharmacyi (Tier 2) does not apply (home covered (home delivery) certificate). nformation/ delivery) $50/prescription, deductible 50% coinsurance up to Typically Non-Preferred Brand does not apply (retail) and $250/prescription, deductible and Generic drugs (Tier 3) $125/prescription, deductible does not apply (retail) and Not does not apply (home covered (home delivery) delivery) * For more information about limitations and exceptions, see the plan or policy document at https://eoc.anthem.com/eocdps/. Page 2 of 12
 Anthem Classic PPO 500/30/50/20 SBC Page 1 Page 3
Anthem Classic PPO 500/30/50/20 SBC Page 1 Page 3