
Anthem Value Ded HMO 2000 30 60 25% Select HMO Summary
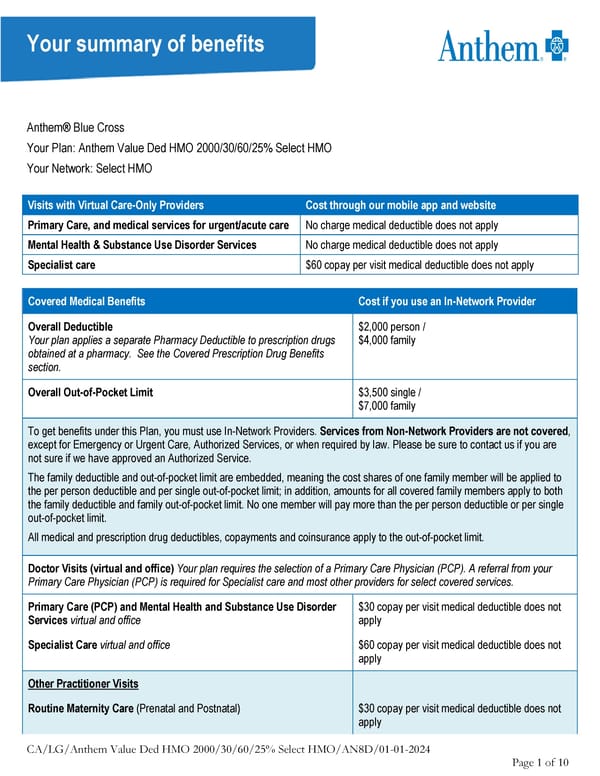
Your summary of benefits Anthem® Blue Cross Your Plan: Anthem Value Ded HMO 2000/30/60/25% Select HMO Your Network: Select HMO Visits with Virtual Care-Only Providers Cost through our mobile app and website Primary Care, and medical services for urgent/acute care No charge medical deductible does not apply Mental Health & Substance Use Disorder Services No charge medical deductible does not apply Specialist care $60 copay per visit medical deductible does not apply Covered Medical Benefits Cost if you use an In-Network Provider Overall Deductible $2,000 person / Your plan applies a separate Pharmacy Deductible to prescription drugs $4,000 family obtained at a pharmacy. See the Covered Prescription Drug Benefits section. Overall Out-of-Pocket Limit $3,500 single / $7,000 family To get benefits under this Plan, you must use In-Network Providers. Services from Non-Network Providers are not covered, except for Emergency or Urgent Care, Authorized Services, or when required by law. Please be sure to contact us if you are not sure if we have approved an Authorized Service. The family deductible and out-of-pocket limit are embedded, meaning the cost shares of one family member will be applied to the per person deductible and per single out-of-pocket limit; in addition, amounts for all covered family members apply to both the family deductible and family out-of-pocket limit. No one member will pay more than the per person deductible or per single out-of-pocket limit. All medical and prescription drug deductibles, copayments and coinsurance apply to the out-of-pocket limit. Doctor Visits (virtual and office) Your plan requires the selection of a Primary Care Physician (PCP). A referral from your Primary Care Physician (PCP) is required for Specialist care and most other providers for select covered services. Primary Care (PCP) and Mental Health and Substance Use Disorder $30 copay per visit medical deductible does not Services virtual and office apply Specialist Care virtual and office $60 copay per visit medical deductible does not apply Other Practitioner Visits Routine Maternity Care (Prenatal and Postnatal) $30 copay per visit medical deductible does not apply CA/LG/Anthem Value Ded HMO 2000/30/60/25% Select HMO/AN8D/01-01-2024 Page 1 of 10
 Anthem Value Ded HMO 2000 30 60 25% Select HMO Summary Page 2
Anthem Value Ded HMO 2000 30 60 25% Select HMO Summary Page 2