
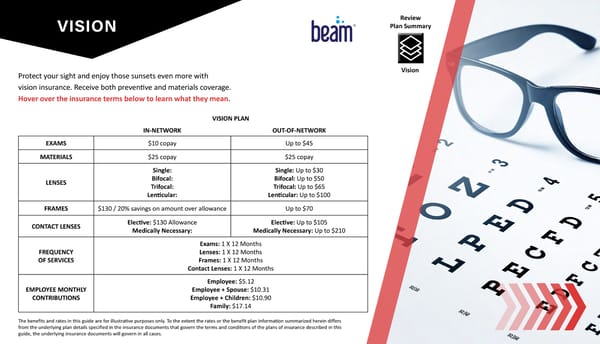
VISION Protect your sight and enjoy those sunsets even more with vision insurance. Receive both preventive and materials coverage. Hover over the insurance terms below to learn what they mean. VISION PLAN IN-NETWORK OUT-OF-NETWORK EXAMS $10 copay Up to $45 MATERIALS $25 copay $25 copay LENSES Single: Bifocal: Trifocal: Lenticular: Single: Up to $30 Bifocal: Up to $50 Trifocal: Up to $65 Lenticular: Up to $100 FRAMES $130 / 20% savings on amount over allowance Up to $70 CONTACT LENSES Elective: $130 Allowance Medically Necessary: Elective: Up to $105 Medically Necessary: Up to $210 FREQUENCY OF SERVICES Exams: 1 X 12 Months Lenses: 1 X 12 Months Frames: 1 X 12 Months Contact Lenses: 1 X 12 Months EMPLOYEE MONTHLY CONTRIBUTIONS Employee: $5.12 Employee + Spouse: $10.31 Employee + Children: $10.90 Family: $17.14 The benefits and rates in this guide are for illustrative purposes only. To the extent the rates or the benefit plan information summarized herein differs from the underlying plan details specified in the insurance documents that govern the terms and conditions of the plans of insurance described in this guide, the underlying insurance documents will govern in all cases. Vision Review Plan Summary
 Dash Delivery Benefits Guide 2026 Page 6 Page 8
Dash Delivery Benefits Guide 2026 Page 6 Page 8