
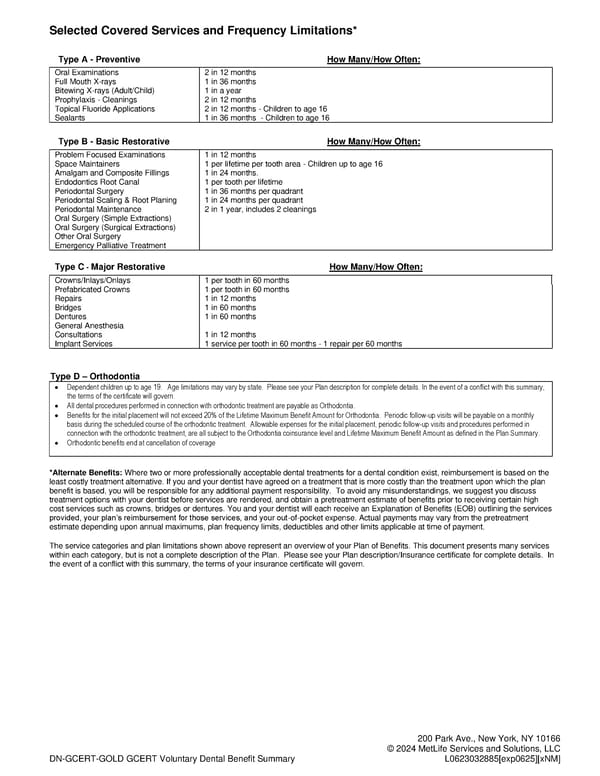
DN-GCERT-GOLD GCERT Voluntary Dental Benefit Summary 200 Park Ave., New York, NY 10166 © 2024 MetLife Services and Solutions, LLC L0623032885[exp0625][xNM] Selected Covered Services and Frequency Limitations* Type A - Preventive How Many/How Often: Oral Examinations 2 in 12 months Full Mouth X-rays 1 in 36 months Bitewing X-rays (Adult/Child) 1 in a year Prophylaxis - Cleanings 2 in 12 months Topical Fluoride Applications 2 in 12 months - Children to age 16 Sealants 1 in 36 months - Children to age 16 Type B - Basic Restorative How Many/How Often: Problem Focused Examinations 1 in 12 months Space Maintainers 1 per lifetime per tooth area - Children up to age 16 Amalgam and Composite Fillings 1 in 24 months. Endodontics Root Canal 1 per tooth per lifetime Periodontal Surgery 1 in 36 months per quadrant Periodontal Scaling & Root Planing 1 in 24 months per quadrant Periodontal Maintenance 2 in 1 year, includes 2 cleanings Oral Surgery (Simple Extractions) Oral Surgery (Surgical Extractions) Other Oral Surgery Emergency Palliative Treatment Type C - Major Restorative How Many/How Often: Crowns/Inlays/Onlays 1 per tooth in 60 months Prefabricated Crowns 1 per tooth in 60 months Repairs 1 in 12 months Bridges 1 in 60 months Dentures 1 in 60 months General Anesthesia Consultations 1 in 12 months Implant Services 1 service per tooth in 60 months - 1 repair per 60 months Type D – Orthodontia • Dependent children up to age 19. Age limitations may vary by state. Please see your Plan description for complete details. In the event of a conflict with this summary, the terms of the certificate will govern. • All dental procedures performed in connection with orthodontic treatment are payable as Orthodontia. • Benefits for the initial placement will not exceed 20% of the Lifetime Maximum Benefit Amount for Orthodontia. Periodic follow-up visits will be payable on a monthly basis during the scheduled course of the orthodontic treatment. Allowable expenses for the initial placement, periodic follow-up visits and procedures performed in connection with the orthodontic treatment, are all subject to the Orthodontia coinsurance level and Lifetime Maximum Benefit Amount as defined in the Plan Summary. • Orthodontic benefits end at cancellation of coverage *Alternate Benefits: Where two or more professionally acceptable dental treatments for a dental condition exist, reimbursement is based on the least costly treatment alternative. If you and your dentist have agreed on a treatment that is more costly than the treatment upon which the plan benefit is based, you will be responsible for any additional payment responsibility. To avoid any misunderstandings, we suggest you discuss treatment options with your dentist before services are rendered, and obtain a pretreatment estimate of benefits prior to receiving certain high cost services such as crowns, bridges or dentures. You and your dentist will each receive an Explanation of Benefits (EOB) outlining the services provided, your plan’s reimbursement for those services, and your out-of-pocket expense. Actual payments may vary from the pretreatment estimate depending upon annual maximums, plan frequency limits, deductibles and other limits applicable at time of payment. The service categories and plan limitations shown above represent an overview of your Plan of Benefits. This document presents many services within each category, but is not a complete description of the Plan. Please see your Plan description/Insurance certificate for complete details. In the event of a conflict with this summary, the terms of your insurance certificate will govern.
 Dental Plan Page 3 Page 5
Dental Plan Page 3 Page 5