
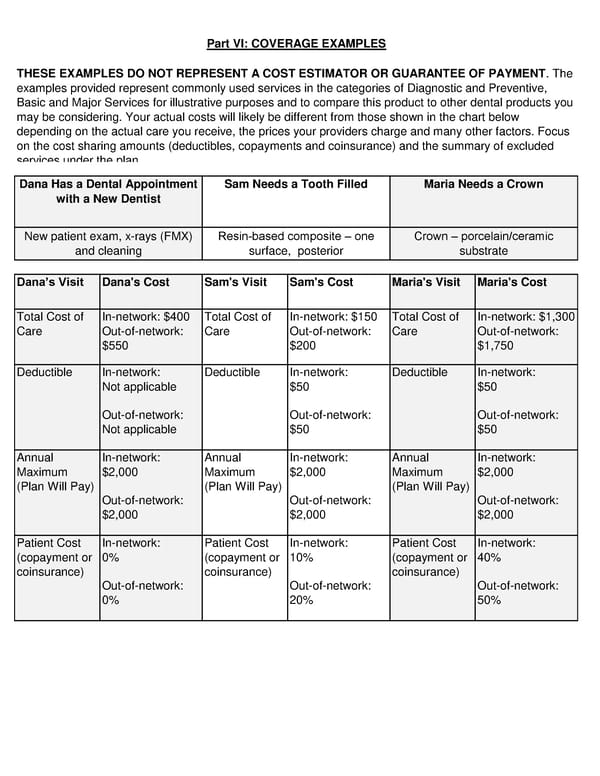
Part VI: COVERAGE EXAMPLES THESE EXAMPLES DO NOT REPRESENT A COST ESTIMATOR OR GUARANTEE OF PAYMENT. The examples provided represent commonly used services in the categories of Diagnostic and Preventive, Basic and Major Services for illustrative purposes and to compare this product to other dental products you may be considering. Your actual costs will likely be different from those shown in the chart below depending on the actual care you receive, the prices your providers charge and many other factors. Focus on the cost sharing amounts (deductibles, copayments and coinsurance) and the summary of excluded services under the plan. Dana Has a Dental Appointment Sam Needs a Tooth Filled Maria Needs a Crown with a New Dentist New patient exam, x-rays (FMX) Resin-based composite – one Crown – porcelain/ceramic and cleaning surface, posterior substrate Dana’s Visit Dana's Cost Sam's Visit Sam's Cost Maria's Visit Maria's Cost Total Cost of In-network: $400 Total Cost of In-network: $150 Total Cost of In-network: $1,300 Care Out-of-network: Care Out-of-network: Care Out-of-network: $550 $200 $1,750 Deductible In-network: Deductible In-network: Deductible In-network: Not applicable $50 $50 Out-of-network: Out-of-network: Out-of-network: Not applicable $50 $50 Annual In-network: Annual In-network: Annual In-network: Maximum $2,000 Maximum $2,000 Maximum $2,000 (Plan Will Pay) (Plan Will Pay) (Plan Will Pay) Out-of-network: Out-of-network: Out-of-network: $2,000 $2,000 $2,000 Patient Cost In-network: Patient Cost In-network: Patient Cost In-network: (copayment or 0% (copayment or 10% (copayment or 40% coinsurance) coinsurance) coinsurance) Out-of-network: Out-of-network: Out-of-network: 0% 20% 50%
 Dental SDBC Page 4 Page 6
Dental SDBC Page 4 Page 6