
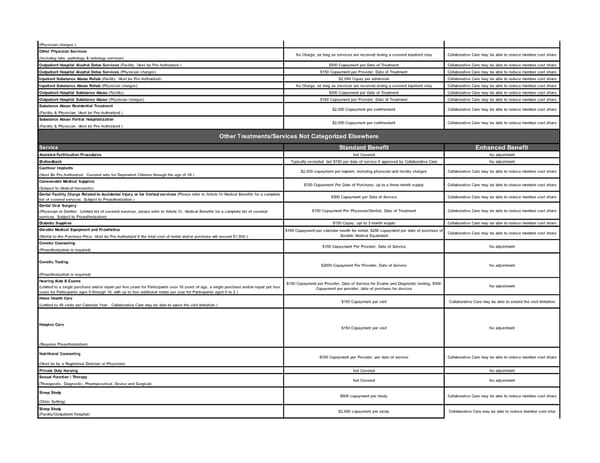
(Physician charges.) Other Physician Services (Including labs, pathology & radiology services) Outpatient Hospital Alcohol Detox Services (Facility. Must be Pre-Authorized.) $500 Copayment per Date of Treatment Collaborative Care may be able to reduce member cost share Outpatient Hospital Alcohol Detox Services (Physician charges) $150 Copayment per Provider, Date of Treatment Collaborative Care may be able to reduce member cost share Inpatient Substance Abuse Rehab (Facility. Must be Pre-Authorized) $2,000 Copay per admission Collaborative Care may be able to reduce member cost share Inpatient Substance Abuse Rehab (Physician charges) No Charge, as long as services are received during a covered inpatient stay Collaborative Care may be able to reduce member cost share Outpatient Hospital Substance Abuse (Facility) $500 Copayment per Date of Treatment Collaborative Care may be able to reduce member cost share Outpatient Hospital Substance Abuse (Physician charges) $150 Copayment per Provider, Date of Treatment Collaborative Care may be able to reduce member cost share Substance Abuse Residential Treatment (Facility & Physician. Must be Pre-Authorized.) Substance Abuse Partial Hospitalization (Facility & Physician. Must be Pre-Authorized.) Service Standard Benefit Enhanced Benefit Assisted Fertilization Procedures Not Covered No adjustment Biofeedback Typically excluded, but $150 per date of service if approved by Collaborative Care No adjustment Cochlear Implants (Must Be Pre-Authorized. Covered only for Dependent Children through the age of 18.) Consumable Medical Supplies (Subject to Medical Necessity) Dental Facility Charge Related to Accidental Injury or for limited services (Please refer to Article III-Medical Benefits for a complete list of covered services. Subject to Preauthorization.) $500 Copayment per Date of Service Collaborative Care may be able to reduce member cost share Dental Oral Surgery (Physician or Dentist. Limited list of covered services, please refer to Article III, Medical Benefits for a complete list of covered services. Subject to Preauthorization) Diabetic Supplies $150 Copay, upt to 3 month supply Collaborative Care may be able to reduce member cost share Durable Medical Equipment and Prosthetics (Rental to the Purchase Price. Must be Pre-Authorized if the total cost of rental and/or purchase will exceed $1,500.) Genetic Counseling (Preauthorization is required) Genetic Testing (Preauthorization is required) Hearing Aids & Exams (Limited to a single purchase and/or repair per five years for Participants over 18 years of age, a single purchase and/or repair per four years for Participants ages 0 through 18, with up to four additional molds per year for Participants aged 0 to 2.) Home Health Care (Limited to 40 visits per Calendar Year. Collaborative Care may be able to waive the visit limitation.) Hospice Care (Requires Preauthorization) Nutritional Counseling (Must be by a Registered Dietician or Physician) Private Duty Nursing Not Covered No adjustment Sexual Function / Therapy (Therapeutic, Diagnostic, Pharmaceutical, Device and Surgical) Sleep Study (Clinic Setting) Sleep Study (Facility/Outpatient Hospital) $2,000 copayment per study Collaborative Care may be able to reduce member cost shar $2,000 Copayment per confinement Collaborative Care may be able to reduce member cost share Other Treatments/Services Not Categorized Elsewhere $2,000 copayment per implant, including physician and facility charges Collaborative Care may be able to reduce member cost share $150 Copayment Per Date of Purchase, up to a three-month supply Collaborative Care may be able to reduce member cost share No Charge, as long as services are received during a covered inpatient stay Collaborative Care may be able to reduce member cost share No Charge, as long as services are received during a covered inpatient stay Collaborative Care may be able to reduce member cost share $2,000 Copayment per confinement Collaborative Care may be able to reduce member cost share $2000 Copayment Per Provider, Date of Service No adjustment $150 Copayment per Provider, Date of Service for Exams and Diagnostic testing, $500 Copayment per provider, date of purchase for devices No adjustment $150 Copayment per visit Collaborative Care may be able to extend the visit limitation $150 Copayment Per Physician/Dentist, Date of Treatment Collaborative Care may be able to reduce member cost share $150 Copayment per calendar month for rental, $250 copayment per date of purchase of Durable Medical Equipment Collaborative Care may be able to reduce member cost share $150 Copayment Per Provider, Date of Service No adjustment $500 copayment per study Collaborative Care may be able to reduce member cost share $150 Copayment per visit No adjustment $150 Copayment per Provider, per date of service Collaborative Care may be able to reduce member cost share Not Covered No adjustment
 Double Cheese SBC Page 4 Page 6
Double Cheese SBC Page 4 Page 6