
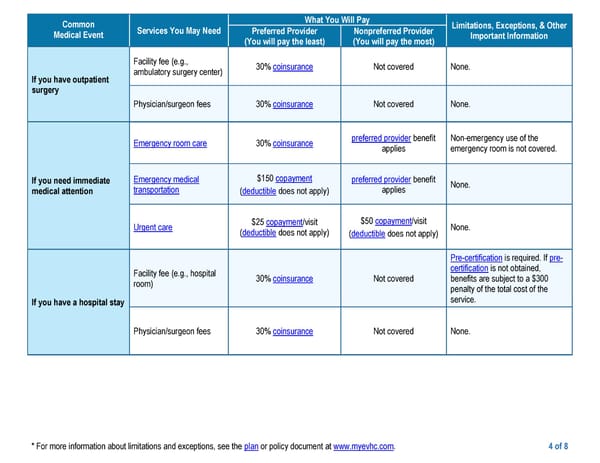
* For more information about limitations and exceptions, see the plan or policy document at www.myevhc.com. 4 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Provider (You will pay the least) Nonpreferred Provider (You will pay the most) If you have outpatient surgery Facility fee (e.g., ambulatory surgery center) 30% coinsurance Not covered None. Physician/surgeon fees 30% coinsurance Not covered None. If you need immediate medical attention Emergency room care 30% coinsurance preferred provider benefit applies Non-emergency use of the emergency room is not covered. Emergency medical transportation $150 copayment (deductible does not apply) preferred provider benefit applies None. Urgent care $25 copayment/visit (deductible does not apply) $50 copayment/visit (deductible does not apply) None. If you have a hospital stay Facility fee (e.g., hospital room) 30% coinsurance Not covered Pre-certification is required. If pre- certification is not obtained, benefits are subject to a $300 penalty of the total cost of the service. Physician/surgeon fees 30% coinsurance Not covered None.
 EPO Page 3 Page 5
EPO Page 3 Page 5