
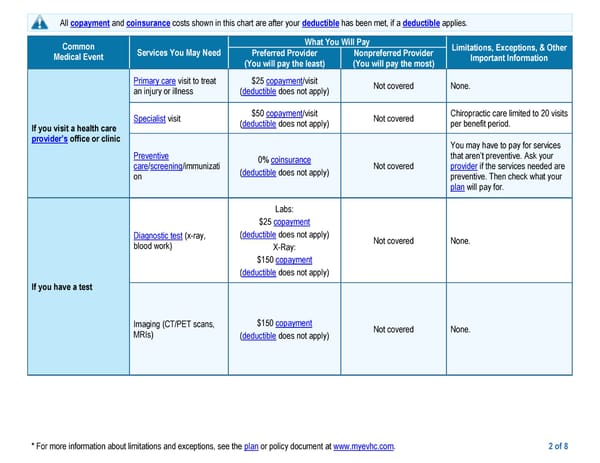
* For more information about limitations and exceptions, see the plan or policy document at www.myevhc.com. 2 of 8 All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Provider (You will pay the least) Nonpreferred Provider (You will pay the most) If you visit a health care provider’s office or clinic Primary care visit to treat an injury or illness $25 copayment/visit (deductible does not apply) Not covered None. Specialist visit $50 copayment/visit (deductible does not apply) Not covered Chiropractic care limited to 20 visits per benefit period. Preventive care/screening/immunizati on 0% coinsurance (deductible does not apply) Not covered You may have to pay for services that aren’t preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. If you have a test Diagnostic test (x-ray, blood work) Labs: $25 copayment (deductible does not apply) X-Ray: $150 copayment (deductible does not apply) Not covered None. Imaging (CT/PET scans, MRIs) $150 copayment (deductible does not apply) Not covered None.
 EPO Page 1 Page 3
EPO Page 1 Page 3