
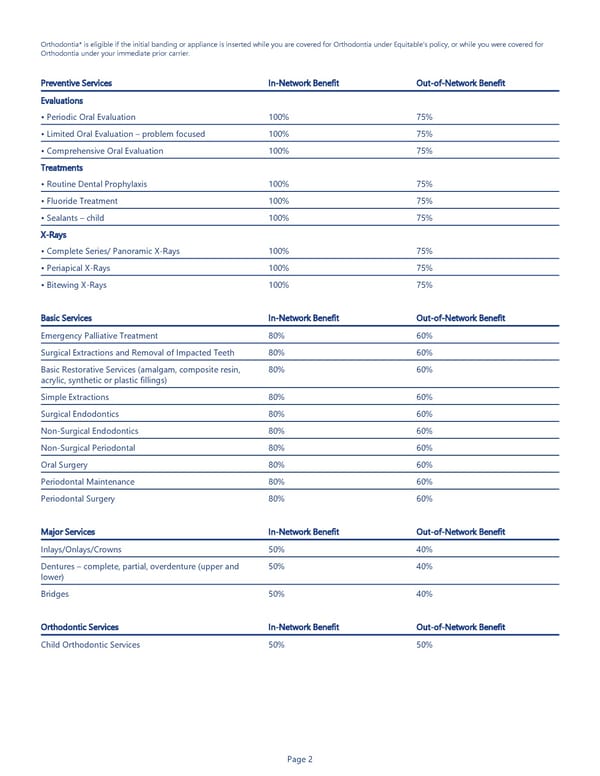
Page 2 Orthodontia* is eligible if the initial banding or appliance is inserted while you are covered for Orthodontia under Equitable’s policy, or while you were covered for Orthodontia under your immediate prior carrier. Preventive Services In-Network Benefit Out-of-Network Benefit Evaluations • Periodic Oral Evaluation 100% 75% • Limited Oral Evaluation – problem focused 100% 75% • Comprehensive Oral Evaluation 100% 75% Treatments • Routine Dental Prophylaxis 100% 75% • Fluoride Treatment 100% 75% • Sealants – child 100% 75% X-Rays • Complete Series/ Panoramic X-Rays 100% 75% • Periapical X-Rays 100% 75% • Bitewing X-Rays 100% 75% Basic Services In-Network Benefit Out-of-Network Benefit Emergency Palliative Treatment 80% 60% Surgical Extractions and Removal of Impacted Teeth 80% 60% Basic Restorative Services (amalgam, composite resin, acrylic, synthetic or plastic fillings) 80% 60% Simple Extractions 80% 60% Surgical Endodontics 80% 60% Non-Surgical Endodontics 80% 60% Non-Surgical Periodontal 80% 60% Oral Surgery 80% 60% Periodontal Maintenance 80% 60% Periodontal Surgery 80% 60% Major Services In-Network Benefit Out-of-Network Benefit Inlays/Onlays/Crowns 50% 40% Dentures – complete, partial, overdenture (upper and lower) 50% 40% Bridges 50% 40% Orthodontic Services In-Network Benefit Out-of-Network Benefit Child Orthodontic Services 50% 50%
 Equitable Dental Insurance Benefit Summary Page 1 Page 3
Equitable Dental Insurance Benefit Summary Page 1 Page 3