
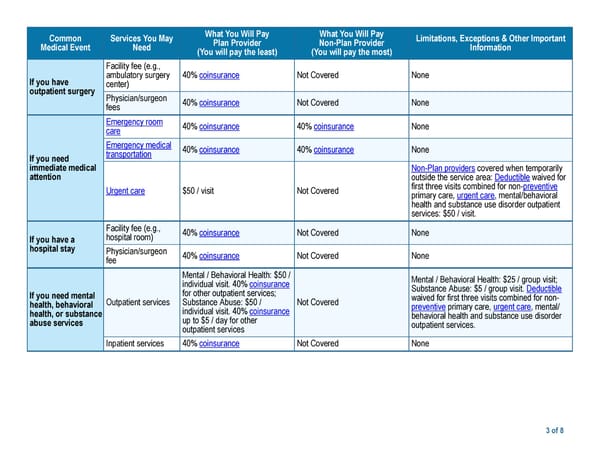
What You Will Pay What You Will Pay Common Services You May Limitations, Exceptions & Other Important Plan Provider Non-Plan Provider Medical Event Need Information (You will pay the least) (You will pay the most) Facility fee (e.g., ambulatory surgery 40% coinsurance Not Covered None If you have center) outpatient surgery Physician/surgeon 40% coinsurance Not Covered None fees Emergency room 40% coinsurance 40% coinsurance None care Emergency medical 40% coinsurance 40% coinsurance None transportation If you need immediate medical Non-Plan providers covered when temporarily attention outside the service area: Deductible waived for first three visits combined for non-preventive Urgent care $50 / visit Not Covered primary care, urgent care, mental/behavioral health and substance use disorder outpatient services: $50 / visit. Facility fee (e.g., 40% coinsurance Not Covered None hospital room) If you have a hospital stay Physician/surgeon 40% coinsurance Not Covered None fee Mental / Behavioral Health: $50 / Mental / Behavioral Health: $25 / group visit; individual visit. 40% coinsurance Substance Abuse: $5 / group visit. Deductible for other outpatient services; If you need mental waived for first three visits combined for non- Outpatient services Substance Abuse: $50 / Not Covered health, behavioral preventive primary care, urgent care, mental/ individual visit. 40% coinsurance health, or substance behavioral health and substance use disorder up to $5 / day for other abuse services outpatient services. outpatient services Inpatient services 40% coinsurance Not Covered None 3 of 8
 Kaiser Permanente DHMO 5500 Southern California SBC Page 2 Page 4
Kaiser Permanente DHMO 5500 Southern California SBC Page 2 Page 4