
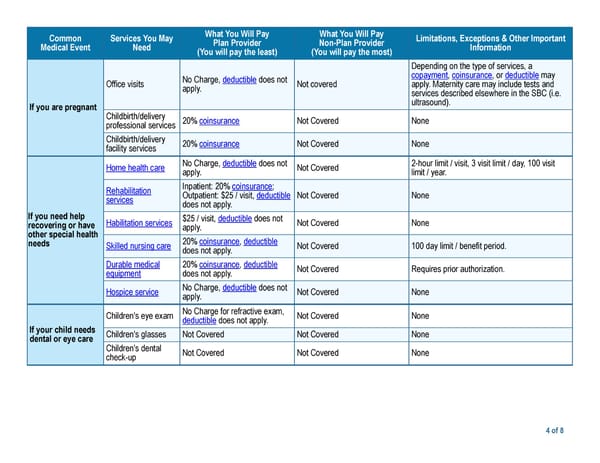
What You Will Pay What You Will Pay Common Services You May Limitations, Exceptions & Other Important Plan Provider Non-Plan Provider Medical Event Need Information (You will pay the least) (You will pay the most) Depending on the type of services, a copayment, coinsurance, or deductible may No Charge, deductible does not Office visits Not covered apply. Maternity care may include tests and apply. services described elsewhere in the SBC (i.e. ultrasound). If you are pregnant Childbirth/delivery 20% coinsurance Not Covered None professional services Childbirth/delivery 20% coinsurance Not Covered None facility services No Charge, deductible does not 2-hour limit / visit, 3 visit limit / day, 100 visit Home health care Not Covered apply. limit / year. Inpatient: 20% coinsurance; Rehabilitation Outpatient: $25 / visit, deductible Not Covered None services does not apply. If you need help $25 / visit, deductible does not Habilitation services Not Covered None recovering or have apply. other special health 20% coinsurance, deductible needs Skilled nursing care Not Covered 100 day limit / benefit period. does not apply. Durable medical 20% coinsurance, deductible Not Covered Requires prior authorization. equipment does not apply. No Charge, deductible does not Hospice service Not Covered None apply. No Charge for refractive exam, Children's eye exam Not Covered None deductible does not apply. If your child needs Children's glasses Not Covered Not Covered None dental or eye care Children's dental Not Covered Not Covered None check-up 4 of 8
 Kaiser Permanente DHMO 750 Northern California SBC Page 3 Page 5
Kaiser Permanente DHMO 750 Northern California SBC Page 3 Page 5