
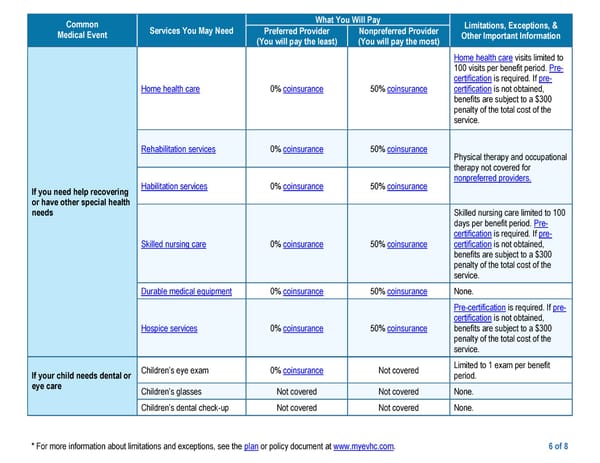
* For more information about limitations and exceptions, see the plan or policy document at www.myevhc.com. 6 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Provider (You will pay the least) Nonpreferred Provider (You will pay the most) If you need help recovering or have other special health needs Home health care 0% coinsurance 50% coinsurance Home health care visits limited to 100 visits per benefit period. Pre- certification is required. If pre- certification is not obtained, benefits are subject to a $300 penalty of the total cost of the service. Rehabilitation services 0% coinsurance 50% coinsurance Physical therapy and occupational therapy not covered for nonpreferred providers. Habilitation services 0% coinsurance 50% coinsurance Skilled nursing care 0% coinsurance 50% coinsurance Skilled nursing care limited to 100 days per benefit period. Pre- certification is required. If pre- certification is not obtained, benefits are subject to a $300 penalty of the total cost of the service. Durable medical equipment 0% coinsurance 50% coinsurance None. Hospice services 0% coinsurance 50% coinsurance Pre-certification is required. If pre- certification is not obtained, benefits are subject to a $300 penalty of the total cost of the service. If your child needs dental or eye care Children’s eye exam 0% coinsurance Not covered Limited to 1 exam per benefit period. Children’s glasses Not covered Not covered None. Children’s dental check-up Not covered Not covered None.
 Medical HDHP Plan Page 5 Page 7
Medical HDHP Plan Page 5 Page 7