
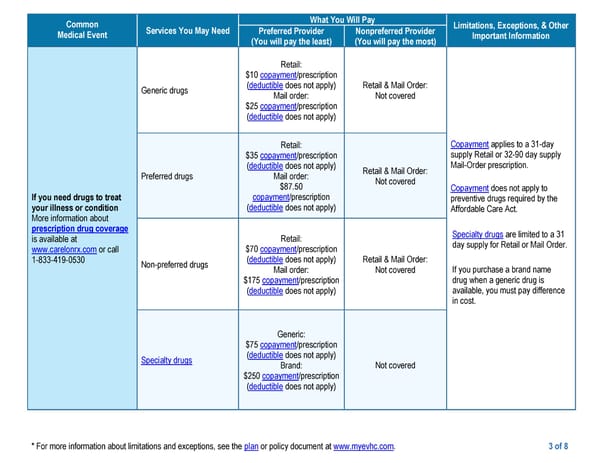
* For more information about limitations and exceptions, see the plan or policy document at www.myevhc.com. 3 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Provider (You will pay the least) Nonpreferred Provider (You will pay the most) If you need drugs to treat your illness or condition More information about prescription drug coverage is available at www.carelonrx.com or call 1-833-419-0530 Generic drugs Retail: $10 copayment/prescription (deductible does not apply) Mail order: $25 copayment/prescription (deductible does not apply) Retail & Mail Order: Not covered Copayment applies to a 31-day supply Retail or 32-90 day supply Mail-Order prescription. Copayment does not apply to preventive drugs required by the Affordable Care Act. Specialty drugs are limited to a 31 day supply for Retail or Mail Order. If you purchase a brand name drug when a generic drug is available, you must pay difference in cost. Preferred drugs Retail: $35 copayment/prescription (deductible does not apply) Mail order: $87.50 copayment/prescription (deductible does not apply) Retail & Mail Order: Not covered Non-preferred drugs Retail: $70 copayment/prescription (deductible does not apply) Mail order: $175 copayment/prescription (deductible does not apply) Retail & Mail Order: Not covered Specialty drugs Generic: $75 copayment/prescription (deductible does not apply) Brand: $250 copayment/prescription (deductible does not apply) Not covered
 Medical PPO Plan Page 2 Page 4
Medical PPO Plan Page 2 Page 4