
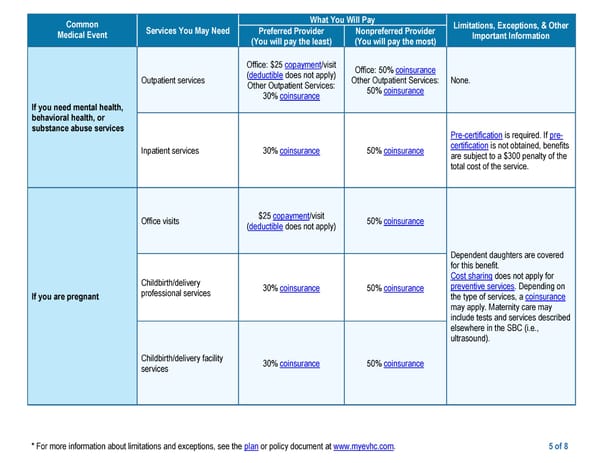
* For more information about limitations and exceptions, see the plan or policy document at www.myevhc.com. 5 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Provider (You will pay the least) Nonpreferred Provider (You will pay the most) If you need mental health, behavioral health, or substance abuse services Outpatient services Office: $25 copayment/visit (deductible does not apply) Other Outpatient Services: 30% coinsurance Office: 50% coinsurance Other Outpatient Services: 50% coinsurance None. Inpatient services 30% coinsurance 50% coinsurance Pre-certification is required. If pre- certification is not obtained, benefits are subject to a $300 penalty of the total cost of the service. If you are pregnant Office visits $25 copayment/visit (deductible does not apply) 50% coinsurance Dependent daughters are covered for this benefit. Cost sharing does not apply for preventive services. Depending on the type of services, a coinsurance may apply. Maternity care may include tests and services described elsewhere in the SBC (i.e., ultrasound). Childbirth/delivery professional services 30% coinsurance 50% coinsurance Childbirth/delivery facility services 30% coinsurance 50% coinsurance
 Medical PPO Plan Page 4 Page 6
Medical PPO Plan Page 4 Page 6