
Salus Healthcare Insurance Plan Comparison
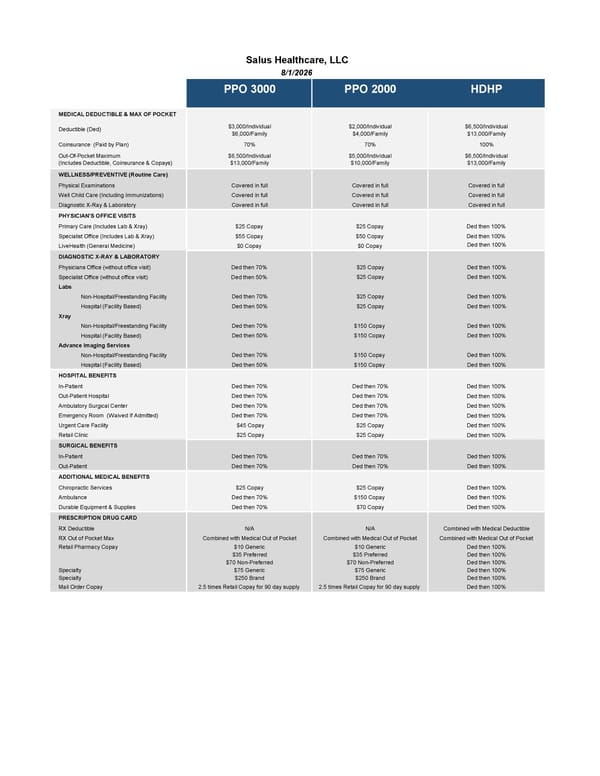
This document provides a detailed comparison of medical benefits, including deductibles, co-pays, and coverage options for different healthcare plans offered by Salus Healthcare as of August 1, 2026.
PPO 3000 PPO 2000 HDHP MEDICAL DEDUCTIBLE & MAX OF POCKET $3,000/Individual $2,000/Individual $6,500/Individual $6,000/Family $4,000/Family $13,000/Family Coinsurance (Paid by Plan) 70% 70% 100% Out-Of-Pocket Maximum $6,500/Individual $5,000/Individual $6,500/Individual (Includes Deductible, Coinsurance & Copays) $13,000/Family $10,000/Family $13,000/Family WELLNESS/PREVENTIVE (Routine Care) Physical Examinations Covered in full Covered in full Covered in full Well Child Care (Including Immunizations) Covered in full Covered in full Covered in full Diagnostic X-Ray & Laboratory Covered in full Covered in full Covered in full PHYSICIAN'S OFFICE VISITS Primary Care (Includes Lab & Xray) $25 Copay $25 Copay Ded then 100% Specialist Office (Includes Lab & Xray) $55 Copay $50 Copay Ded then 100% LiveHealth (General Medicine) $0 Copay $0 Copay Ded then 100% DIAGNOSTIC X-RAY & LABORATORY Physicians Office (without office visit) Ded then 70% $25 Copay Ded then 100% Specialist Office (without office visit) Ded then 50% $25 Copay Ded then 100% Labs Non-Hospital/Freestanding Facility Ded then 70% $25 Copay Ded then 100% Hospital (Facility Based) Ded then 50% $25 Copay Ded then 100% Xray Non-Hospital/Freestanding Facility Ded then 70% $150 Copay Ded then 100% Hospital (Facility Based) Ded then 50% $150 Copay Ded then 100% Advance Imaging Services Non-Hospital/Freestanding Facility Ded then 70% $150 Copay Ded then 100% Hospital (Facility Based) Ded then 50% $150 Copay Ded then 100% HOSPITAL BENEFITS In-Patient Ded then 70% Ded then 70% Ded then 100% Out-Patient Hospital Ded then 70% Ded then 70% Ded then 100% Ambulatory Surgical Center Ded then 70% Ded then 70% Ded then 100% Emergency Room (Waived If Admitted) Ded then 70% Ded then 70% Ded then 100% Urgent Care Facility $45 Copay $25 Copay Ded then 100% Retail Clinic $25 Copay $25 Copay Ded then 100% SURGICAL BENEFITS In-Patient Ded then 70% Ded then 70% Ded then 100% Out-Patient Ded then 70% Ded then 70% Ded then 100% ADDITIONAL MEDICAL BENEFITS Chiropractic Services $25 Copay $25 Copay Ded then 100% Ambulance Ded then 70% $150 Copay Ded then 100% Durable Equipment & Supplies Ded then 70% $70 Copay Ded then 100% PRESCRIPTION DRUG CARD RX Deductible N/A N/A Combined with Medical Deductible RX Out of Pocket Max Combined with Medical Out of Pocket Combined with Medical Out of Pocket Combined with Medical Out of Pocket Retail Pharmacy Copay $10 Generic $10 Generic Ded then 100% $35 Preferred $35 Preferred Ded then 100% $70 Non-Preferred $70 Non-Preferred Ded then 100% Specialty $75 Generic $75 Generic Ded then 100% Specialty $250 Brand $250 Brand Ded then 100% Mail Order Copay 2.5 times Retail Copay for 90 day supply 2.5 times Retail Copay for 90 day supply Ded then 100% Deductible (Ded) Salus Healthcare, LLC 8/1/2026
 Salus Healthcare Insurance Plan Comparison
Salus Healthcare Insurance Plan Comparison