
Schedule of Benefits
This document outlines the covered services, co-payment details, and appointment guidelines for plan members and their dependents under the MetLife Direct Referral Dental Plan.
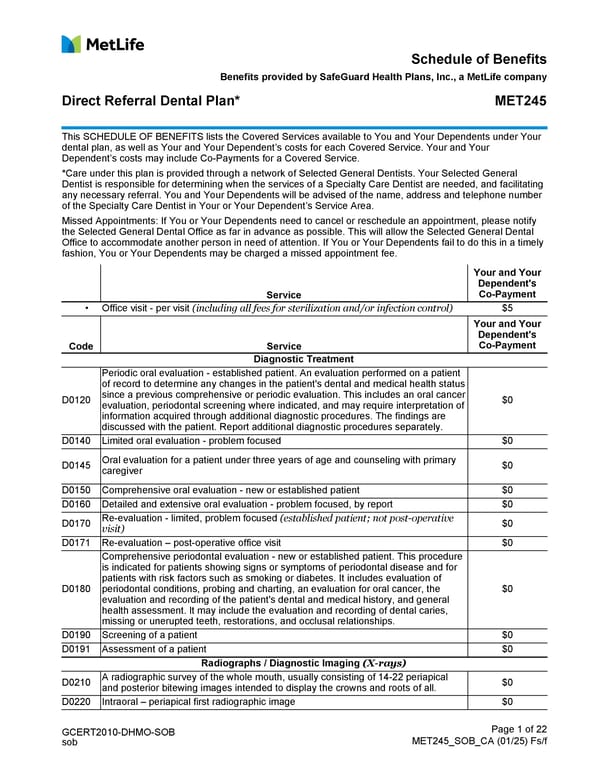
GCERT2010-DHMO-SOB sob Page 1 of 22 MET245_SOB_CA (01/25) Fs/f Schedule of Benefits Benefits provided by SafeGuard Health Plans, Inc., a MetLife company Direct Referral Dental Plan* MET245 This SCHEDULE OF BENEFITS lists the Covered Services available to You and Your Dependents under Your dental plan, as well as Your and Your Dependent’s costs for each Covered Service. Your and Your Dependent’s costs may include Co-Payments for a Covered Service. *Care under this plan is provided through a network of Selected General Dentists. Your Selected General Dentist is responsible for determining when the services of a Specialty Care Dentist are needed, and facilitating any necessary referral. You and Your Dependents will be advised of the name, address and telephone number of the Specialty Care Dentist in Your or Your Dependent’s Service Area. Missed Appointments: If You or Your Dependents need to cancel or reschedule an appointment, please notify the Selected General Dental Office as far in advance as possible. This will allow the Selected General Dental Office to accommodate another person in need of attention. If You or Your Dependents fail to do this in a timely fashion, You or Your Dependents may be charged a missed appointment fee. Service Your and Your Dependent's Co-Payment • Office visit - per visit (including all fees for sterilization and/or infection control) $5 Code Service Your and Your Dependent's Co-Payment Diagnostic Treatment D0120 Periodic oral evaluation - established patient. An evaluation performed on a patient of record to determine any changes in the patient's dental and medical health status since a previous comprehensive or periodic evaluation. This includes an oral cancer evaluation, periodontal screening where indicated, and may require interpretation of information acquired through additional diagnostic procedures. The findings are discussed with the patient. Report additional diagnostic procedures separately. $0 D0140 Limited oral evaluation - problem focused $0 D0145 Oral evaluation for a patient under three years of age and counseling with primary caregiver $0 D0150 Comprehensive oral evaluation - new or established patient $0 D0160 Detailed and extensive oral evaluation - problem focused, by report $0 D0170 Re-evaluation - limited, problem focused (established patient; not post-operative visit) $0 D0171 Re-evaluation – post-operative office visit $0 D0180 Comprehensive periodontal evaluation - new or established patient. This procedure is indicated for patients showing signs or symptoms of periodontal disease and for patients with risk factors such as smoking or diabetes. It includes evaluation of periodontal conditions, probing and charting, an evaluation for oral cancer, the evaluation and recording of the patient's dental and medical history, and general health assessment. It may include the evaluation and recording of dental caries, missing or unerupted teeth, restorations, and occlusal relationships. $0 D0190 Screening of a patient $0 D0191 Assessment of a patient $0 Radiographs / Diagnostic Imaging (X-rays) D0210 A radiographic survey of the whole mouth, usually consisting of 14-22 periapical and posterior bitewing images intended to display the crowns and roots of all. $0 D0220 Intraoral – periapical first radiographic image $0
 Schedule of Benefits Page 2
Schedule of Benefits Page 2