
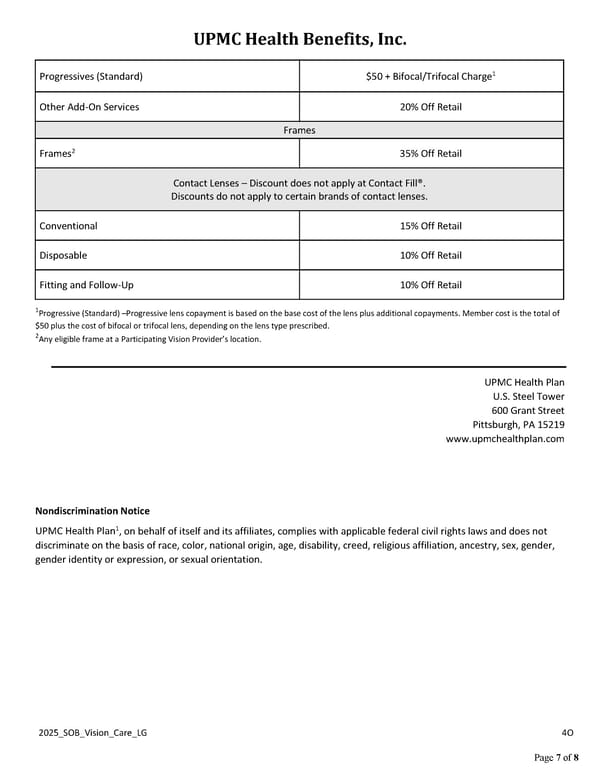
UPMC Health Benefits, Inc. 2025_SOB_Vision_Care_LG 4O Page 7 of 8 Progressives (Standard) $50 + Bifocal/Trifocal Charge1 Other Add-On Services 20% Off Retail Frames Frames2 35% Off Retail Contact Lenses – Discount does not apply at Contact Fill®. Discounts do not apply to certain brands of contact lenses. Conventional 15% Off Retail Disposable 10% Off Retail Fitting and Follow-Up 10% Off Retail 1Progressive (Standard) –Progressive lens copayment is based on the base cost of the lens plus additional copayments. Member cost is the total of $50 plus the cost of bifocal or trifocal lens, depending on the lens type prescribed. 2Any eligible frame at a Participating Vision Provider’s location. UPMC Health Plan U.S. Steel Tower 600 Grant Street Pittsburgh, PA 15219 www.upmchealthplan.com Nondiscrimination Notice UPMC Health Plan1, on behalf of itself and its affiliates, complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, creed, religious affiliation, ancestry, sex, gender, gender identity or expression, or sexual orientation.
 UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 6 Page 8
UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 6 Page 8