
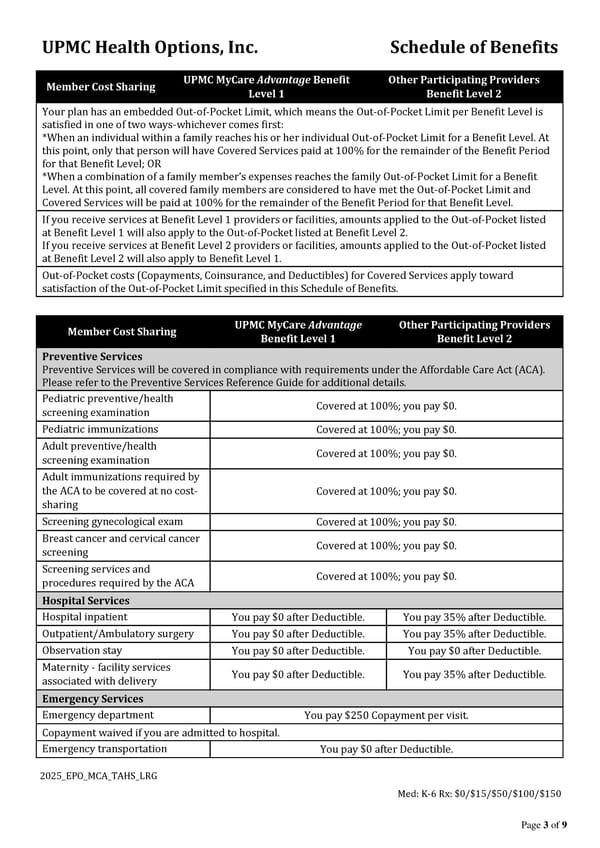
UPMC Health Options, Inc. Schedule of Benefits 2025_EPO_MCA_TAHS_LRG Med: K-6 Rx: $0/$15/$50/$100/$150 Page 3 of 9 Member Cost Sharing UPMC MyCare Advantage Benefit Level 1 Other Participating Providers Benefit Level 2 Your plan has an embedded Out-of-Pocket Limit, which means the Out-of-Pocket Limit per Benefit Level is satisfied in one of two ways-whichever comes first: *When an individual within a family reaches his or her individual Out-of-Pocket Limit for a Benefit Level. At this point, only that person will have Covered Services paid at 100% for the remainder of the Benefit Period for that Benefit Level; OR *When a combination of a family member’s expenses reaches the family Out-of-Pocket Limit for a Benefit Level. At this point, all covered family members are considered to have met the Out-of-Pocket Limit and Covered Services will be paid at 100% for the remainder of the Benefit Period for that Benefit Level. If you receive services at Benefit Level 1 providers or facilities, amounts applied to the Out-of-Pocket listed at Benefit Level 1 will also apply to the Out-of-Pocket listed at Benefit Level 2. If you receive services at Benefit Level 2 providers or facilities, amounts applied to the Out-of-Pocket listed at Benefit Level 2 will also apply to Benefit Level 1. Out-of-Pocket costs (Copayments, Coinsurance, and Deductibles) for Covered Services apply toward satisfaction of the Out-of-Pocket Limit specified in this Schedule of Benefits. Member Cost Sharing UPMC MyCare Advantage Benefit Level 1 Other Participating Providers Benefit Level 2 Preventive Services Preventive Services will be covered in compliance with requirements under the Affordable Care Act (ACA). Please refer to the Preventive Services Reference Guide for additional details. Pediatric preventive/health screening examination Covered at 100%; you pay $0. Pediatric immunizations Covered at 100%; you pay $0. Adult preventive/health screening examination Covered at 100%; you pay $0. Adult immunizations required by the ACA to be covered at no cost- sharing Covered at 100%; you pay $0. Screening gynecological exam Covered at 100%; you pay $0. Breast cancer and cervical cancer screening Covered at 100%; you pay $0. Screening services and procedures required by the ACA Covered at 100%; you pay $0. Hospital Services Hospital inpatient You pay $0 after Deductible. You pay 35% after Deductible. Outpatient/Ambulatory surgery You pay $0 after Deductible. You pay 35% after Deductible. Observation stay You pay $0 after Deductible. You pay $0 after Deductible. Maternity - facility services associated with delivery You pay $0 after Deductible. You pay 35% after Deductible. Emergency Services Emergency department You pay $250 Copayment per visit. Copayment waived if you are admitted to hospital. Emergency transportation You pay $0 after Deductible.
 UPMC Health Options: Schedule of Benefits Page 2 Page 4
UPMC Health Options: Schedule of Benefits Page 2 Page 4