
UPMC Health Options Schedule of Benefits
This document outlines the benefits and copayment details for UPMC Health Options, including deductibles, coinsurance, and specific healthcare service costs.
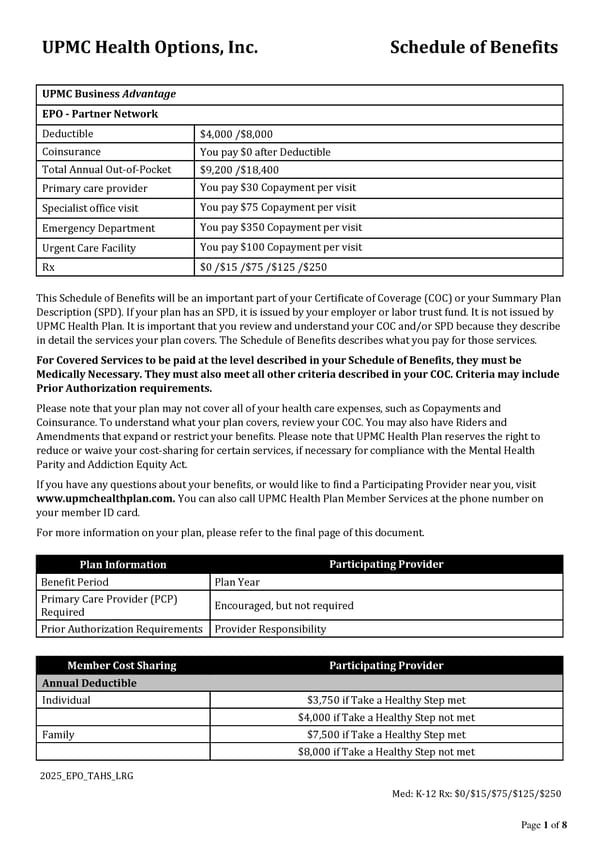
UPMC Health Options, Inc. Schedule of Benefits 2025_EPO_TAHS_LRG Med: K-12 Rx: $0/$15/$75/$125/$250 Page 1 of 8 UPMC Business Advantage EPO - Partner Network Deductible $4,000 /$8,000 Coinsurance You pay $0 after Deductible Total Annual Out-of-Pocket $9,200 /$18,400 Primary care provider You pay $30 Copayment per visit Specialist office visit You pay $75 Copayment per visit Emergency Department You pay $350 Copayment per visit Urgent Care Facility You pay $100 Copayment per visit Rx $0 /$15 /$75 /$125 /$250 This Schedule of Benefits will be an important part of your Certificate of Coverage (COC) or your Summary Plan Description (SPD). If your plan has an SPD, it is issued by your employer or labor trust fund. It is not issued by UPMC Health Plan. It is important that you review and understand your COC and/or SPD because they describe in detail the services your plan covers. The Schedule of Benefits describes what you pay for those services. For Covered Services to be paid at the level described in your Schedule of Benefits, they must be Medically Necessary. They must also meet all other criteria described in your COC. Criteria may include Prior Authorization requirements. Please note that your plan may not cover all of your health care expenses, such as Copayments and Coinsurance. To understand what your plan covers, review your COC. You may also have Riders and Amendments that expand or restrict your benefits. Please note that UPMC Health Plan reserves the right to reduce or waive your cost-sharing for certain services, if necessary for compliance with the Mental Health Parity and Addiction Equity Act. If you have any questions about your benefits, or would like to find a Participating Provider near you, visit www.upmchealthplan.com. You can also call UPMC Health Plan Member Services at the phone number on your member ID card. For more information on your plan, please refer to the final page of this document. Plan Information Participating Provider Benefit Period Plan Year Primary Care Provider (PCP) Required Encouraged, but not required Prior Authorization Requirements Provider Responsibility Member Cost Sharing Participating Provider Annual Deductible Individual $3,750 if Take a Healthy Step met $4,000 if Take a Healthy Step not met Family $7,500 if Take a Healthy Step met $8,000 if Take a Healthy Step not met
 UPMC Health Options Schedule of Benefits Page 2
UPMC Health Options Schedule of Benefits Page 2