
Vision Summary
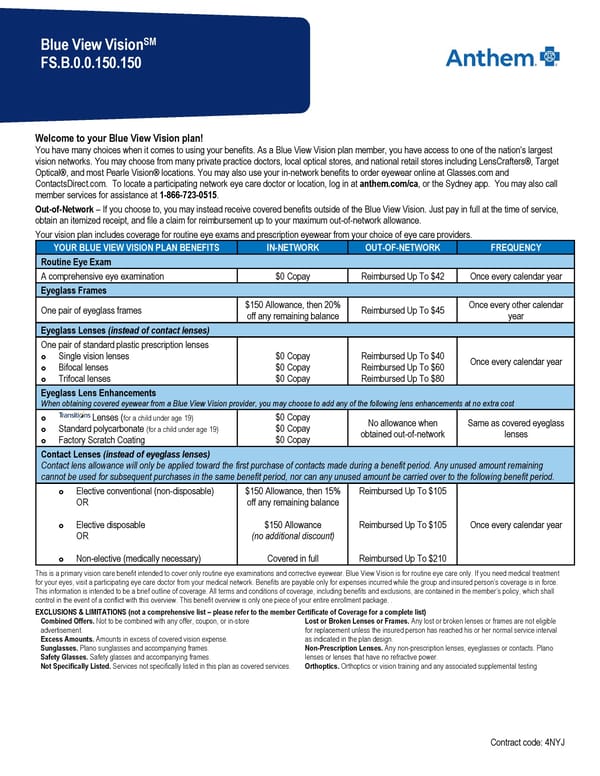
SM Blue View Vision FS.B.0.0.150.150 Welcome to your Blue View Vision plan! You have many choices when it comes to using your benefits. As a Blue View Vision plan member, you have access to one of the nation’s largest vision networks. You may choose from many private practice doctors, local optical stores, and national retail stores including LensCrafters®, Target Optical®, and most Pearle Vision® locations. You may also use your in-network benefits to order eyewear online at Glasses.com and ContactsDirect.com. To locate a participating network eye care doctor or location, log in at anthem.com/ca, or the Sydney app. You may also call member services for assistance at 1-866-723-0515. Out-of-Network – If you choose to, you may instead receive covered benefits outside of the Blue View Vision. Just pay in full at the time of service, obtain an itemized receipt, and file a claim for reimbursement up to your maximum out-of-network allowance. Your vision plan includes coverage for routine eye exams and prescription eyewear from your choice of eye care providers. YOUR BLUE VIEW VISION PLAN BENEFITS IN-NETWORK OUT-OF-NETWORK FREQUENCY Routine Eye Exam A comprehensive eye examination $0 Copay Reimbursed Up To $42 Once every calendar year Eyeglass Frames One pair of eyeglass frames $150 Allowance, then 20% Reimbursed Up To $45 Once every other calendar off any remaining balance year Eyeglass Lenses (instead of contact lenses) One pair of standard plastic prescription lenses Single vision lenses $0 Copay Reimbursed Up To $40 Once every calendar year Bifocal lenses $0 Copay Reimbursed Up To $60 Trifocal lenses $0 Copay Reimbursed Up To $80 Eyeglass Lens Enhancements When obtaining covered eyewear from a Blue View Vision provider, you may choose to add any of the following lens enhancements at no extra cost Lenses (for a child under age 19) $0 Copay No allowance when Same as covered eyeglass Standard polycarbonate (for a child under age 19) $0 Copay obtained out-of-network lenses Factory Scratch Coating $0 Copay Contact Lenses (instead of eyeglass lenses) Contact lens allowance will only be applied toward the first purchase of contacts made during a benefit period. Any unused amount remaining cannot be used for subsequent purchases in the same benefit period, nor can any unused amount be carried over to the following benefit period. Elective conventional (non-disposable) $150 Allowance, then 15% Reimbursed Up To $105 OR off any remaining balance Elective disposable $150 Allowance Reimbursed Up To $105 Once every calendar year OR (no additional discount) Non-elective (medically necessary) Covered in full Reimbursed Up To $210 This is a primary vision care benefit intended to cover only routine eye examinations and corrective eyewear. Blue View Vision is for routine eye care only. If you need medical treatment for your eyes, visit a participating eye care doctor from your medical network. Benefits are payable only for expenses incurred while the group and insured person’s coverage is in force. This information is intended to be a brief outline of coverage. All terms and conditions of coverage, including benefits and exclusions, are contained in the member’s policy, which shall control in the event of a conflict with this overview. This benefit overview is only one piece of your entire enrollment package. . EXCLUSIONS & LIMITATIONS (not a comprehensive list – please refer to the member Certificate of Coverage for a complete list) Combined Offers. Not to be combined with any offer, coupon, or in-store Lost or Broken Lenses or Frames. Any lost or broken lenses or frames are not eligible advertisement. for replacement unless the insured person has reached his or her normal service interval Excess Amounts. Amounts in excess of covered vision expense. as indicated in the plan design. Sunglasses. Plano sunglasses and accompanying frames. Non-Prescription Lenses. Any non-prescription lenses, eyeglasses or contacts. Plano Safety Glasses. Safety glasses and accompanying frames. lenses or lenses that have no refractive power. Not Specifically Listed. Services not specifically listed in this plan as covered services. Orthoptics. Orthoptics or vision training and any associated supplemental testing Contract code: 4NYJ
 Vision Summary Page 2
Vision Summary Page 2