
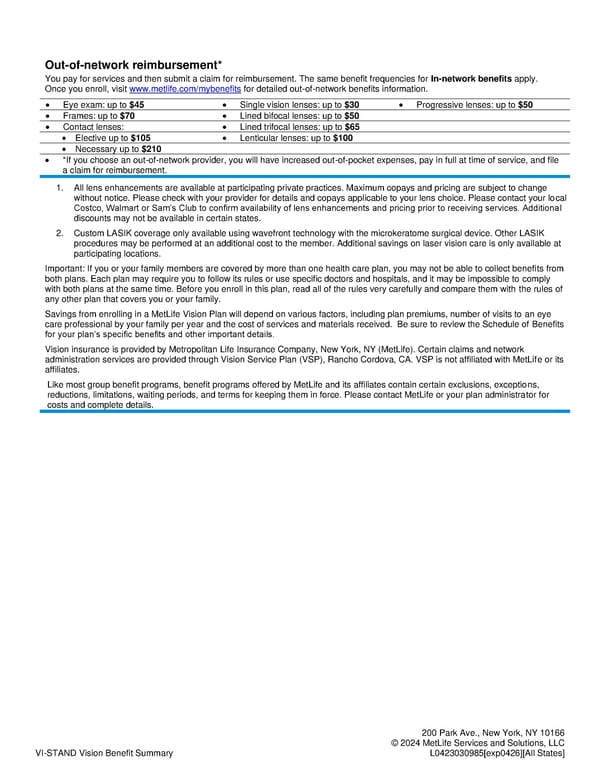
VI-STAND Vision Benefit Summary 200 Park Ave., New York, NY 10166 © 2024 MetLife Services and Solutions, LLC L0423030985[exp0426][All States] Out-of-network reimbursement* You pay for services and then submit a claim for reimbursement. The same benefit frequencies for In-network benefits apply. Once you enroll, visit www.metlife.com/mybenefits for detailed out-of-network benefits information. • Eye exam: up to $45 • Single vision lenses: up to $30 • Progressive lenses: up to $50 • Frames: up to $70 • Lined bifocal lenses: up to $50 • Contact lenses: • Lined trifocal lenses: up to $65 • Elective up to $105 • Lenticular lenses: up to $100 • Necessary up to $210 • *If you choose an out-of-network provider, you will have increased out-of-pocket expenses, pay in full at time of service, and file a claim for reimbursement. 1. All lens enhancements are available at participating private practices. Maximum copays and pricing are subject to change without notice. Please check with your provider for details and copays applicable to your lens choice. Please contact your local Costco, Walmart or Sam’s Club to confirm availability of lens enhancements and pricing prior to receiving services. Additional discounts may not be available in certain states. 2. Custom LASIK coverage only available using wavefront technology with the microkeratome surgical device. Other LASIK procedures may be performed at an additional cost to the member. Additional savings on laser vision care is only available at participating locations. Important: If you or your family members are covered by more than one health care plan, you may not be able to collect benefits from both plans. Each plan may require you to follow its rules or use specific doctors and hospitals, and it may be impossible to comply with both plans at the same time. Before you enroll in this plan, read all of the rules very carefully and compare them with the rules of any other plan that covers you or your family. Savings from enrolling in a MetLife Vision Plan will depend on various factors, including plan premiums, number of visits to an eye care professional by your family per year and the cost of services and materials received. Be sure to review the Schedule of Benefits for your plan’s specific benefits and other important details. Vision insurance is provided by Metropolitan Life Insurance Company, New York, NY (MetLife). Certain claims and network administration services are provided through Vision Service Plan (VSP), Rancho Cordova, CA. VSP is not affiliated with MetLife or its affiliates. Like most group benefit programs, benefit programs offered by MetLife and its affiliates contain certain exclusions, exceptions, reductions, limitations, waiting periods, and terms for keeping them in force. Please contact MetLife or your plan administrator for costs and complete details.
 VSP Choice Page 1 Page 3
VSP Choice Page 1 Page 3