
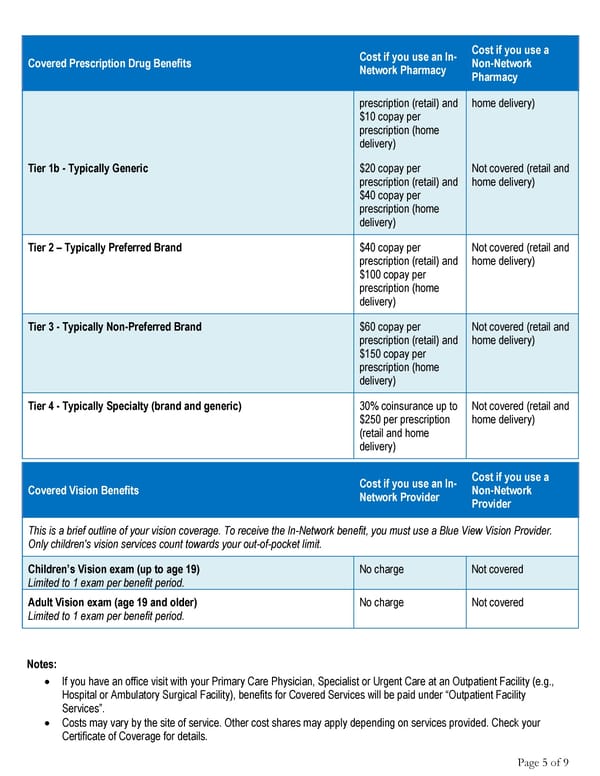
Cost if you use an In- Cost if you use a Covered Prescription Drug Benefits Network Pharmacy Non-Network Pharmacy prescription (retail) and home delivery) $10 copay per prescription (home delivery) Tier 1b - Typically Generic $20 copay per Not covered (retail and prescription (retail) and home delivery) $40 copay per prescription (home delivery) Tier 2 – Typically Preferred Brand $40 copay per Not covered (retail and prescription (retail) and home delivery) $100 copay per prescription (home delivery) Tier 3 - Typically Non-Preferred Brand $60 copay per Not covered (retail and prescription (retail) and home delivery) $150 copay per prescription (home delivery) Tier 4 - Typically Specialty (brand and generic) 30% coinsurance up to Not covered (retail and $250 per prescription home delivery) (retail and home delivery) Cost if you use an In- Cost if you use a Covered Vision Benefits Network Provider Non-Network Provider This is a brief outline of your vision coverage. To receive the In-Network benefit, you must use a Blue View Vision Provider. Only children's vision services count towards your out-of-pocket limit. Children’s Vision exam (up to age 19) No charge Not covered Limited to 1 exam per benefit period. Adult Vision exam (age 19 and older) No charge Not covered Limited to 1 exam per benefit period. Notes: • If you have an office visit with your Primary Care Physician, Specialist or Urgent Care at an Outpatient Facility (e.g., Hospital or Ambulatory Surgical Facility), benefits for Covered Services will be paid under “Outpatient Facility Services”. • Costs may vary by the site of service. Other cost shares may apply depending on services provided. Check your Certificate of Coverage for details. Page 5 of 9
 Anthem EPO 3000/25/50/20 Summary Page 4 Page 6
Anthem EPO 3000/25/50/20 Summary Page 4 Page 6