
Dental SDBC
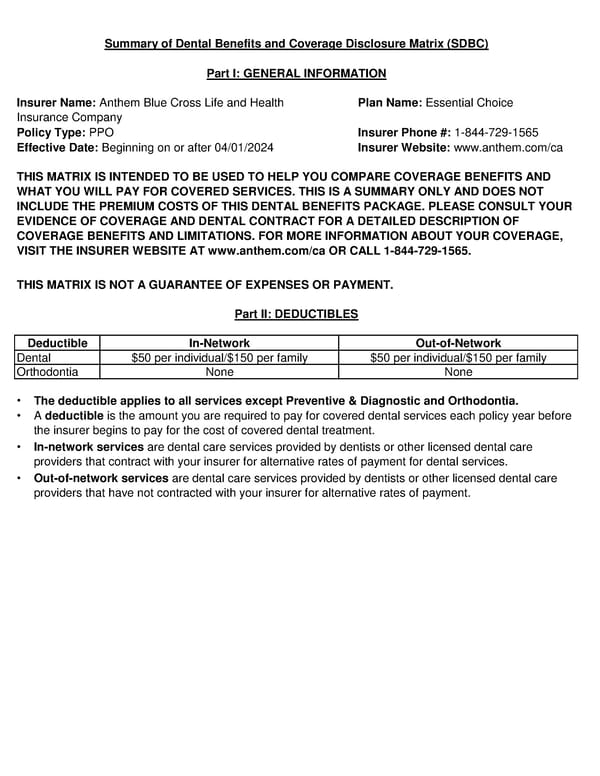
Summary of Dental Benefits and Coverage Disclosure Matrix (SDBC) Part I: GENERAL INFORMATION Insurer Name: Anthem Blue Cross Life and Health Plan Name: Essential Choice Insurance Company Policy Type: PPO Insurer Phone #: 1-844-729-1565 Effective Date: Beginning on or after 04/01/2024 Insurer Website: www.anthem.com/ca THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND WHAT YOU WILL PAY FOR COVERED SERVICES. THIS IS A SUMMARY ONLY AND DOES NOT INCLUDE THE PREMIUM COSTS OF THIS DENTAL BENEFITS PACKAGE. PLEASE CONSULT YOUR EVIDENCE OF COVERAGE AND DENTAL CONTRACT FOR A DETAILED DESCRIPTION OF COVERAGE BENEFITS AND LIMITATIONS. FOR MORE INFORMATION ABOUT YOUR COVERAGE, VISIT THE INSURER WEBSITE AT www.anthem.com/ca OR CALL 1-844-729-1565. THIS MATRIX IS NOT A GUARANTEE OF EXPENSES OR PAYMENT. Part II: DEDUCTIBLES Deductible In-Network Out-of-Network Dental $50 per individual/$150 per family $50 per individual/$150 per family Orthodontia None None • The deductible applies to all services except Preventive & Diagnostic and Orthodontia. • A deductible is the amount you are required to pay for covered dental services each policy year before the insurer begins to pay for the cost of covered dental treatment. • In-network services are dental care services provided by dentists or other licensed dental care providers that contract with your insurer for alternative rates of payment for dental services. • Out-of-network services are dental care services provided by dentists or other licensed dental care providers that have not contracted with your insurer for alternative rates of payment.
 Dental SDBC Page 2
Dental SDBC Page 2