
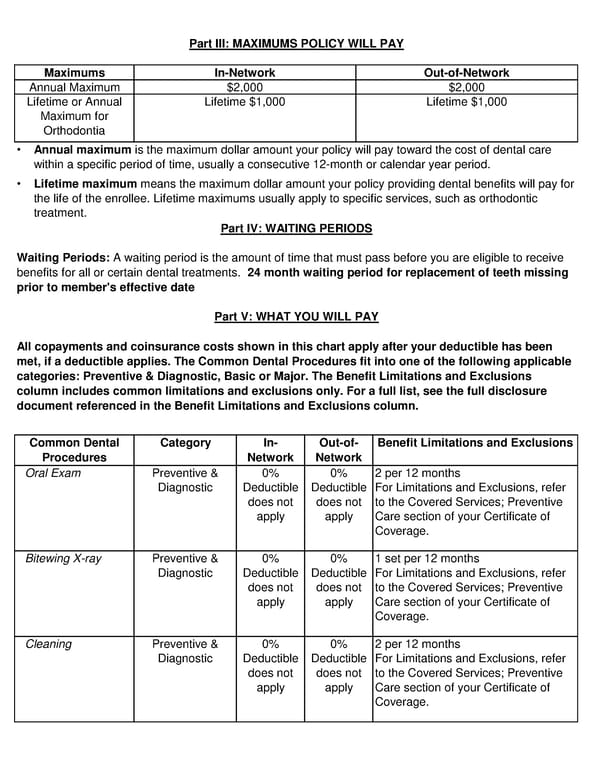
Part III: MAXIMUMS POLICY WILL PAY Maximums In-Network Out-of-Network Annual Maximum $2,000 $2,000 Lifetime or Annual Lifetime $1,000 Lifetime $1,000 Maximum for Orthodontia • Annual maximum is the maximum dollar amount your policy will pay toward the cost of dental care within a specific period of time, usually a consecutive 12-month or calendar year period. • Lifetime maximum means the maximum dollar amount your policy providing dental benefits will pay for the life of the enrollee. Lifetime maximums usually apply to specific services, such as orthodontic treatment. Part IV: WAITING PERIODS Waiting Periods: A waiting period is the amount of time that must pass before you are eligible to receive benefits for all or certain dental treatments. 24 month waiting period for replacement of teeth missing prior to member's effective date Part V: WHAT YOU WILL PAY All copayments and coinsurance costs shown in this chart apply after your deductible has been met, if a deductible applies. The Common Dental Procedures fit into one of the following applicable categories: Preventive & Diagnostic, Basic or Major. The Benefit Limitations and Exclusions column includes common limitations and exclusions only. For a full list, see the full disclosure document referenced in the Benefit Limitations and Exclusions column. Common Dental Category In- Out-of- Benefit Limitations and Exclusions Procedures Network Network Oral Exam Preventive & 0% 0% 2 per 12 months Diagnostic Deductible Deductible For Limitations and Exclusions, refer does not does not to the Covered Services; Preventive apply apply Care section of your Certificate of Coverage. Bitewing X-ray Preventive & 0% 0% 1 set per 12 months Diagnostic Deductible Deductible For Limitations and Exclusions, refer does not does not to the Covered Services; Preventive apply apply Care section of your Certificate of Coverage. Cleaning Preventive & 0% 0% 2 per 12 months Diagnostic Deductible Deductible For Limitations and Exclusions, refer does not does not to the Covered Services; Preventive apply apply Care section of your Certificate of Coverage.
 Dental SDBC Page 1 Page 3
Dental SDBC Page 1 Page 3