
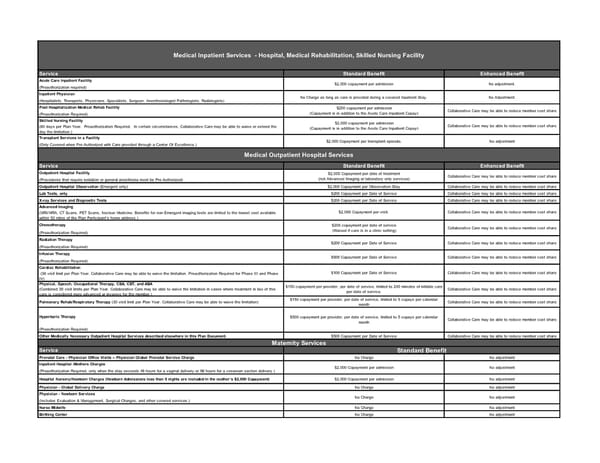
Service Standard Benefit Enhanced Benefit Acute Care Inpatient Facility (Preauthorization required) Inpatient Physician (Hospitalists, Therapists, Physicians, Specialists, Surgeon, Anesthesiologist Pathologists, Radiologists) Post Hospitalization Medical Rehab Facility (Preauthorization Required) Skilled Nursing Facility (60 days per Plan Year. Preauthorization Required. In certain circumstances, Collaborative Care may be able to waive or extend the day the limitation.) Transplant Services in a Facility (Only Covered when Pre-Authorized with Care provided through a Center Of Excellence.) Service Standard Benefit Enhanced Benefit Outpatient Hospital Facility (Procedures that require sedation or general anesthesia must be Pre-Authorized) Outpatient Hospital Observation (Emergent only) $2,000 Copayment per Observation Stay Collaborative Care may be able to reduce member cost share Lab Tests, only $200 Copayment per Date of Service Collaborative Care may be able to reduce member cost share X-ray Services and Diagnostic Tests $200 Copayment per Date of Service Collaborative Care may be able to reduce member cost share Advanced Imaging (MRI/MRA, CT Scans, PET Scans, Nuclear Medicine. Benefits for non-Emergent imaging tests are limited to the lowest cost available within 50 miles of the Plan Participant’s home address.) Chemotherapy (Preauthorization Required) Radiation Therapy (Preauthorization Required) Infusion Therapy (Preauthorization Required) Cardiac Rehabilitation (36 visit limit per Plan Year. Collaborative Care may be able to waive the limitation. Preauthorization Required for Phase III and Phase IV) Physical, Speech, Occupational Therapy, CBA, CBT, and ABA (Combined 30 visit limits per Plan Year. Collaborative Care may be able to waive the limitation in cases where treatment in lieu of this care is considered more advanced or invasive for the member.) $150 copayment per provider, per date of service, limited to 240 minutes of billable care per date of service. Collaborative Care may be able to reduce member cost share Pulmonary Rehab/Respiratory Therapy (30 visit limit per Plan Year. Collaborative Care may be able to waive the limitation) $150 copayment per provider, per date of service, limited to 5 copays per calendar month Collaborative Care may be able to reduce member cost share Hyperbaric Therapy (Preauthorization Required) Other Medically Necessary Outpatient Hospital Services described elsewhere in this Plan Document. $500 Copayment per Date of Service Collaborative Care may be able to reduce member cost share Service Prenatal Care - Physician Office Visits – Physician Global Prenatal Service Charge No Charge No adjustment Inpatient Hospital /Mothers Charges (Preauthorization Required, only when the stay exceeds 48 hours for a vaginal delivery or 96 hours for a cesarean section delivery.) Hospital Nursery/Newborn Charges (Newborn Admissions less than 5 nights are included in the mother’s $2,000 Copayment) $2,000 Copayment per admission No adjustment Physician - Global Delivery Charge No Charge No adjustment Physician - Newborn Services (Includes Evaluation & Management, Surgical Charges, and other covered services.) Nurse Midwife No Charge No adjustment Birthing Center No Charge No adjustment Medical Inpatient Services - Hospital, Medical Rehabilitation, Skilled Nursing Facility $2,000 copayment per admission No adjustment. No Charge as long as care is provided during a covered Inpatient Stay. No Adjustment. Medical Outpatient Hospital Services $2,000 Copayment per date of treatment (not Advanced Imaging or laboratory only services) Collaborative Care may be able to reduce member cost share $2,000 Copayment per visit. Collaborative Care may be able to reduce member cost share $200 copayment per admission (Copayment is in addition to the Acute Care Inpatient Copay) Collaborative Care may be able to reduce member cost share $2,000 copayment per admission (Copayment is in addition to the Acute Care Inpatient Copay) Collaborative Care may be able to reduce member cost share $2,000 Copayment per transplant episode. No adjustment $500 copayment per provider, per date of service, limited to 5 copays per calendar month Collaborative Care may be able to reduce member cost share Maternity Services Standard Benefit $100 Copayment per Date of Service Collaborative Care may be able to reduce member cost share $200 copayment per date of service (Waived if care is in a clinic setting) Collaborative Care may be able to reduce member cost share $200 Copayment per Date of Service Collaborative Care may be able to reduce member cost share $500 Copayment per Date of Service Collaborative Care may be able to reduce member cost share $2,000 Copayment per admission No adjustment No Charge No adjustment
 Double Cheese SBC Page 2 Page 4
Double Cheese SBC Page 2 Page 4