
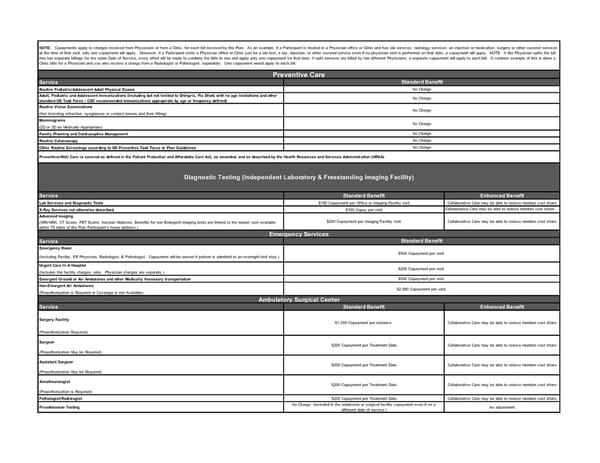
Service Routine Pediatric/Adolescent Adult Physical Exams Adult, Pediatric and Adolescent Immunizations (including but not limited to Shingrix, Flu Shots with no age limitations and other standard US Task Force / CDC recommended Immunizations appropriate by age or frequency defined) Routine Vision Examinations (Not Including refraction, eyeglasses or contact lenses and their fitting) Mammograms (2D or 3D as Medically Appropriate) Family Planning and Contraceptive Management Routine Colonoscopy Other Routine Screenings according to US Preventive Task Force or Plan Guidelines Service Standard Benefit Enhanced Benefit Lab Services and Diagnostic Tests $100 Copayment per Office or Imaging Facility visit Collaborative Care may be able to reduce member cost share X-Ray Services not otherwise described $100 Copay per visit Collaborative Care may be able to reduce member cost share Advanced Imaging (MRI/MRA, CT Scans, PET Scans, Nuclear Medicine. Benefits for non-Emergent imaging tests are limited to the lowest cost available within 75 miles of the Plan Participant’s home address.) Service Emergency Room (Including Facility, ER Physician, Radiologist, & Pathologist. Copayment will be waived if patient is admitted to an overnight bed stay.) Urgent Care In A Hospital (Includes the facility charges, only. Physician charges are separate.) Emergent Ground or Air Ambulance and other Medically Necessary transportation Non-Emergent Air Ambulance (Preauthorization is Required or Coverage is not Available) Service Standard Benefit Enhanced Benefit Surgery Facility (Preauthorization Required) Surgeon (Preauthorization May be Required) Assistant Surgeon (Preauthorization May be Required) Anesthesiologist (Preauthorization is Required) Pathologist/Radiologist $200 Copayment per Treatment Date Collaborative Care may be able to reduce member cost share Preadmission Testing No Charge. (included in the admission or surgical facility copayment even if on a different date of service.) No adjustment Standard Benefit No Charge No Charge No Charge No Charge No Charge NOTE: Copayments apply to charges received from Physicians or from a Clinic, for each bill received by the Plan. As an example, if a Participant is treated in a Physician office or Clinic and has lab services, radiology services, an injection or medication, surgery or other covered services at the time of that visit, only one copayment will apply. Moreover, if a Participant visits a Physician office or Clinic just for a lab test, x-ray, injection, or other covered service even if no physician visit is performed on that date, a copayment will apply. NOTE: It the Physician splits the bill into two separate billings for the same Date of Service, every effort will be made to combine the bills to one and apply only one copayment for that date. If split services are billed by two different Physicians, a separate copayment will apply to each bill. A common example of this is when a Clinic bills for a Physician and you also receive a charge from a Radiologist or Pathologist, separately. One copayment would apply to each bill. Preventive Care Emergency Services Standard Benefit $500 Copayment per visit. $200 Copayment per visit. $500 Copayment per visit. $2,000 Copayment per visit. No Charge No Charge Preventive/Well Care is covered as defined in the Patient Protection and Affordable Care Act, as amended, and as described by the Health Resources and Services Administration (HRSA) Diagnostic Testing (Independent Laboratory & Freestanding Imaging Facility) $200 Copayment per Imaging Facility visit Collaborative Care may be able to reduce member cost share $200 Copayment per Treatment Date Collaborative Care may be able to reduce member cost share Ambulatory Surgical Center $1,000 Copayment per instance. Collaborative Care may be able to reduce member cost share $200 Copayment per Treatment Date Collaborative Care may be able to reduce member cost share $200 Copayment per Treatment Date Collaborative Care may be able to reduce member cost share
 Double Cheese SBC Page 1 Page 3
Double Cheese SBC Page 1 Page 3