
Double Cheese SBC
A detailed overview of standard and enhanced health insurance benefits, including deductible information, out-of-pocket maximums, and specific services offered.
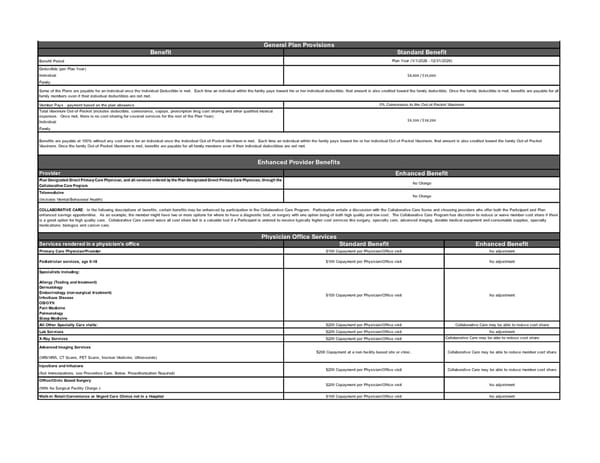
Benefit Benefit Period Deductible (per Plan Year) Individual Family Member Pays - payment based on the plan allowance Total Maximum Out-of-Pocket (includes deductible, coinsurance, copays, prescription drug cost sharing and other qualified medical expenses. Once met, there is no cost sharing for covered services for the rest of the Plan Year). Individual Family Provider Plan Designated Direct Primary Care Physician, and all services ordered by the Plan Designated Direct Primary Care Physician, through the Collaborative Care Program Telemedicine (Includes Mental/Behavioral Health) Services rendered in a physician’s office Standard Benefit Enhanced Benefit Primary Care Physician/Provider $100 Copayment per Physician/Office visit No adjustment Specialists Including: Allergy (Testing and treatment) Dermatology Endocrinology (non-surgical treatment) Infectious Disease OB/GYN Pain Medicine Pulmonology Sleep Medicine $100 Copayment per Physician/Office visit No adjustment All Other Specialty Care visits: $200 Copayment per Physician/Office visit Collaborative Care may be able to reduce cost share Lab Services $200 Copayment per Physician/Office visit No adjustment X-Ray Services $200 Copayment per Physician/Office visit Collaborative Care may be able to reduce cost share Advanced Imaging Services (MRI/MRA, CT Scans, PET Scans, Nuclear Medicine, Ultrasounds) Injections and Infusions (Not Immunizations, see Preventive Care, Below. Preauthorization Required) Office/Clinic Based Surgery (With No Surgical Facility Charge.) Walk-In Retail/Convenience or Urgent Care Clinics not in a Hospital $100 Copayment per Physician/Office visit No adjustment General Plan Provisions Standard Benefit Plan Year (1/1/2026 –12/31/2026) $8,000 / $16,000 Some of the Plans are payable for an individual once the Individual Deductible is met. Each time an individual within the family pays toward his or her individual deductible, that amount is also credited toward the family deductible. Once the family deductible is met, benefits are payable for all family members even if their individual deductibles are not met. 0% Coinsurance to the Out-of-Pocket Maximum COLLABORATIVE CARE : In the following descriptions of benefits, certain benefits may be enhanced by participation in the Collaborative Care Program. Participation entails a discussion with the Collaborative Care Nurse and choosing providers who offer both the Participant and Plan enhanced savings opportunities. As an example, the member might have two or more options for where to have a diagnostic test, or surgery with one option being of both high quality and low cost. The Collaborative Care Program has discretion to reduce or waive member cost share if there is a great option for high quality care. Collaborative Care cannot waive all cost share but is a valuable tool if a Participant is ordered to receive typically higher cost services like surgery, specialty care, advanced imaging, durable medical equipment and consumable supplies, specialty medications, biologics and cancer care. Physician Office Services $200 Copayment at a non-facility-based site or clinic. Collaborative Care may be able to reduce member cost share Pediatrician services, age 0-18 $100 Copayment per Physician/Office visit No adjustment $9,100 / $18,200 Benefits are payable at 100% without any cost share for an individual once the Individual Out-of-Pocket Maximum is met. Each time an individual within the family pays toward his or her individual Out-of-Pocket Maximum, that amount is also credited toward the family Out-of-Pocket Maximum. Once the family Out-of-Pocket Maximum is met, benefits are payable for all family members even if their individual deductibles are not met. Enhanced Provider Benefits Enhanced Benefit No Charge No Charge $200 Copayment per Physician/Office visit Collaborative Care may be able to reduce member cost share $200 Copayment per Physician/Office visit No adjustment
 Double Cheese SBC Page 2
Double Cheese SBC Page 2