
Hospital Indemnity Benefits Summary
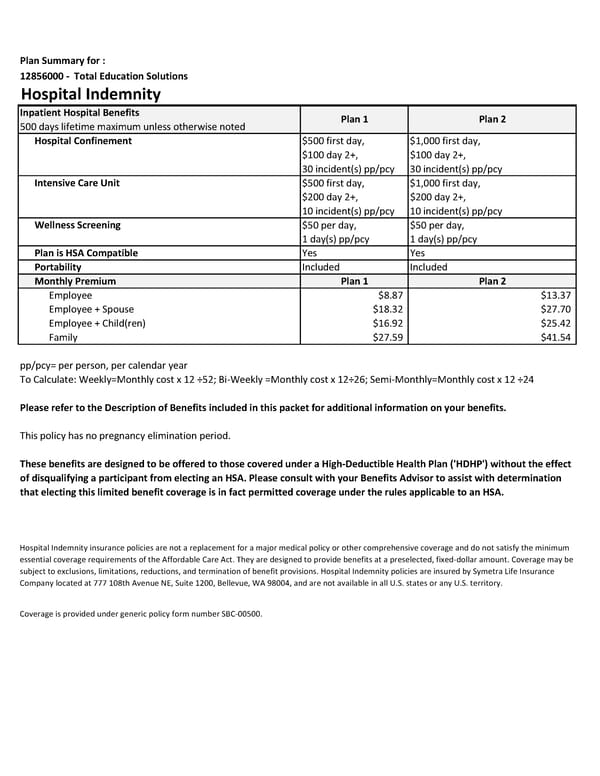
Plan Summary for : 12856000 - Total Education Solutions Hospital Indemnity Inpatient Hospital Benefits Plan 1 Plan 2 500 days lifetime maximum unless otherwise noted Hospital Confinement $500 first day, $1,000 first day, $100 day 2+, $100 day 2+, 30 incident(s) pp/pcy 30 incident(s) pp/pcy Intensive Care Unit $500 first day, $1,000 first day, $200 day 2+, $200 day 2+, 10 incident(s) pp/pcy 10 incident(s) pp/pcy Wellness Screening $50 per day, $50 per day, 1 day(s) pp/pcy 1 day(s) pp/pcy Plan is HSA Compatible Yes Yes Portability Included Included Monthly Premium Plan 1 Plan 2 Employee $8.87 $13.37 Employee + Spouse $18.32 $27.70 Employee + Child(ren) $16.92 $25.42 Family $27.59 $41.54 pp/pcy= per person, per calendar year To Calculate: Weekly=Monthly cost x 12 ÷52; Bi-Weekly =Monthly cost x 12÷26; Semi-Monthly=Monthly cost x 12 ÷24 Please refer to the Description of Benefits included in this packet for additional information on your benefits. This policy has no pregnancy elimination period. These benefits are designed to be offered to those covered under a High-Deductible Health Plan ('HDHP') without the effect of disqualifying a participant from electing an HSA. Please consult with your Benefits Advisor to assist with determination that electing this limited benefit coverage is in fact permitted coverage under the rules applicable to an HSA. Hospital Indemnity insurance policies are not a replacement for a major medical policy or other comprehensive coverage and do not satisfy the minimum essential coverage requirements of the Affordable Care Act. They are designed to provide benefits at a preselected, fixed-dollar amount. Coverage may be subject to exclusions, limitations, reductions, and termination of benefit provisions. Hospital Indemnity policies are insured by Symetra Life Insurance Company located at 777 108th Avenue NE, Suite 1200, Bellevue, WA 98004, and are not available in all U.S. states or any U.S. territory. Coverage is provided under generic policy form number SBC-00500.
 Hospital Indemnity Benefits Summary Page 2
Hospital Indemnity Benefits Summary Page 2