
Kaiser Permanente Traditional HMO Plan Benefits
This document outlines the principal benefits and costs associated with the Kaiser Permanente Traditional HMO Plan, including details about coverage, copayments, and deductibles for various medical services and treatments.
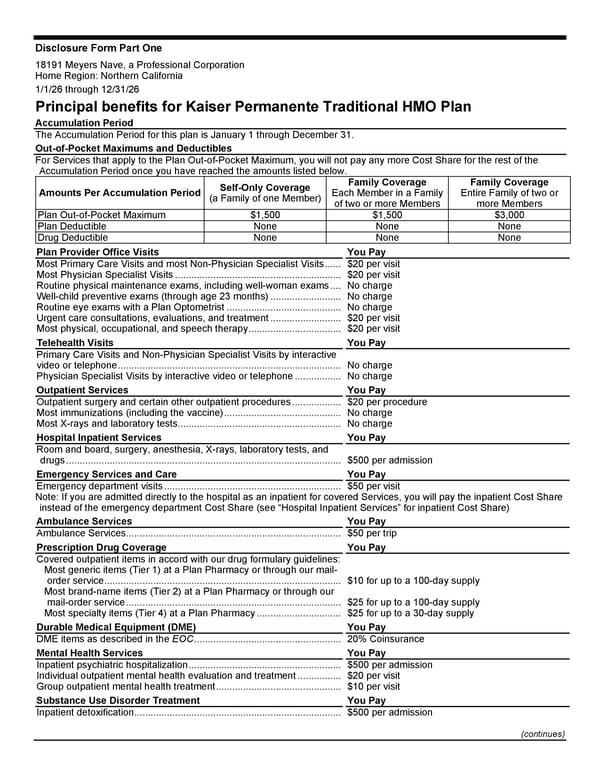
Disclosure Form Part One (continues) 18191 Meyers Nave, a Professional Corporation Home Region: Northern California 1/1/26 through 12/31/26 Principal benefits for Kaiser Permanente Traditional HMO Plan Accumulation Period The Accumulation Period for this plan is January 1 through December 31. Out-of-Pocket Maximums and Deductibles For Services that apply to the Plan Out-of-Pocket Maximum, you will not pay any more Cost Share for the rest of the Accumulation Period once you have reached the amounts listed below. Amounts Per Accumulation Period Self-Only Coverage (a Family of one Member) Family Coverage Each Member in a Family of two or more Members Family Coverage Entire Family of two or more Members Plan Out-of-Pocket Maximum $1,500 $1,500 $3,000 Plan Deductible None None None Drug Deductible None None None Plan Provider Office Visits You Pay Most Primary Care Visits and most Non-Physician Specialist Visits ...... $20 per visit Most Physician Specialist Visits ............................................................. $20 per visit Routine physical maintenance exams, including well-woman exams .... No charge Well-child preventive exams (through age 23 months) .......................... No charge Routine eye exams with a Plan Optometrist .......................................... No charge Urgent care consultations, evaluations, and treatment .......................... $20 per visit Most physical, occupational, and speech therapy .................................. $20 per visit Telehealth Visits You Pay Primary Care Visits and Non-Physician Specialist Visits by interactive video or telephone .................................................................................. No charge Physician Specialist Visits by interactive video or telephone ................. No charge Outpatient Services You Pay Outpatient surgery and certain other outpatient procedures .................. $20 per procedure Most immunizations (including the vaccine) ........................................... No charge Most X-rays and laboratory tests ............................................................ No charge Hospital Inpatient Services You Pay Room and board, surgery, anesthesia, X-rays, laboratory tests, and drugs ..................................................................................................... $500 per admission Emergency Services and Care You Pay Emergency department visits ................................................................. $50 per visit Note: If you are admitted directly to the hospital as an inpatient for covered Services, you will pay the inpatient Cost Share instead of the emergency department Cost Share (see “Hospital Inpatient Services” for inpatient Cost Share) Ambulance Services You Pay Ambulance Services ............................................................................... $50 per trip Prescription Drug Coverage You Pay Covered outpatient items in accord with our drug formulary guidelines: Most generic items (Tier 1) at a Plan Pharmacy or through our mail- order service ....................................................................................... $10 for up to a 100-day supply Most brand-name items (Tier 2) at a Plan Pharmacy or through our mail-order service ............................................................................... $25 for up to a 100-day supply Most specialty items (Tier 4) at a Plan Pharmacy ............................... $25 for up to a 30-day supply Durable Medical Equipment (DME) You Pay DME items as described in the EOC ...................................................... 20% Coinsurance Mental Health Services You Pay Inpatient psychiatric hospitalization ........................................................ $500 per admission Individual outpatient mental health evaluation and treatment ................ $20 per visit Group outpatient mental health treatment .............................................. $10 per visit Substance Use Disorder Treatment You Pay Inpatient detoxification ............................................................................ $500 per admission
 Kaiser Permanente Traditional HMO Plan Benefits Page 2
Kaiser Permanente Traditional HMO Plan Benefits Page 2