
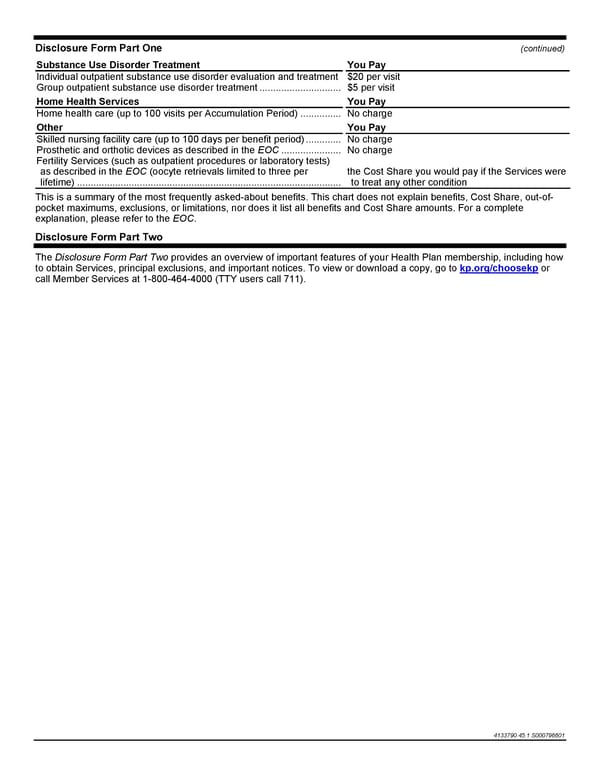
Disclosure Form Part One (continued) 4133790.45.1.S000796601 Substance Use Disorder Treatment You Pay Individual outpatient substance use disorder evaluation and treatment $20 per visit Group outpatient substance use disorder treatment .............................. $5 per visit Home Health Services You Pay Home health care (up to 100 visits per Accumulation Period) ............... No charge Other You Pay Skilled nursing facility care (up to 100 days per benefit period) ............. No charge Prosthetic and orthotic devices as described in the EOC ...................... No charge Fertility Services (such as outpatient procedures or laboratory tests) as described in the EOC (oocyte retrievals limited to three per lifetime) ................................................................................................. the Cost Share you would pay if the Services were to treat any other condition This is a summary of the most frequently asked-about benefits. This chart does not explain benefits, Cost Share, out-of- pocket maximums, exclusions, or limitations, nor does it list all benefits and Cost Share amounts. For a complete explanation, please refer to the EOC. Disclosure Form Part Two The Disclosure Form Part Two provides an overview of important features of your Health Plan membership, including how to obtain Services, principal exclusions, and important notices. To view or download a copy, go to kp.org/choosekp or call Member Services at 1-800-464-4000 (TTY users call 711).
 Kaiser Permanente Traditional HMO Plan Benefits Page 1
Kaiser Permanente Traditional HMO Plan Benefits Page 1