
UPMC Health Benefits: Deluxe Plus Vision Coverage Summary
This document outlines the vision benefits, including examinations and eyewear reimbursements, under the Deluxe Plus $0 Copay plan from UPMC Health Benefits.
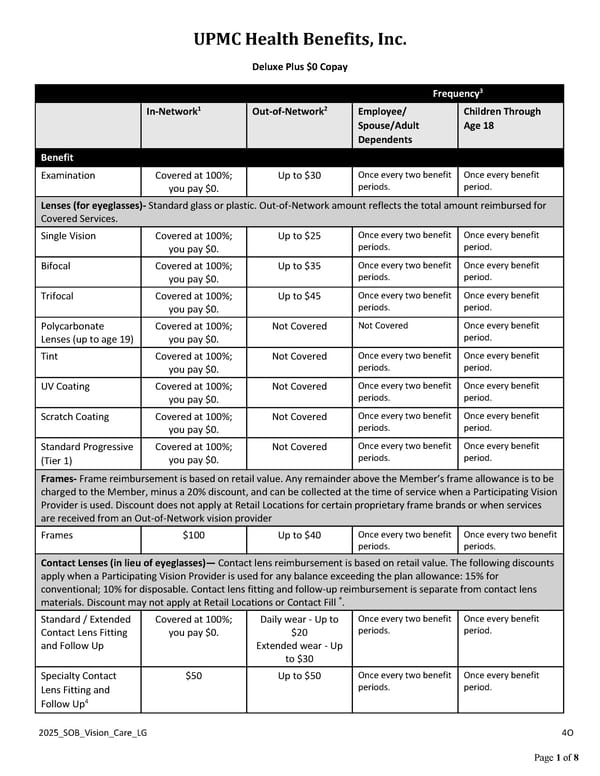
UPMC Health Benefits, Inc. 2025_SOB_Vision_Care_LG 4O Page 1 of 8 Deluxe Plus $0 Copay Frequency3 In-Network1 Out-of-Network2 Employee/ Spouse/Adult Dependents Children Through Age 18 Benefit Examination Covered at 100%; you pay $0. Up to $30 Once every two benefit periods. Once every benefit period. Lenses (for eyeglasses)- Standard glass or plastic. Out-of-Network amount reflects the total amount reimbursed for Covered Services. Single Vision Covered at 100%; you pay $0. Up to $25 Once every two benefit periods. Once every benefit period. Bifocal Covered at 100%; you pay $0. Up to $35 Once every two benefit periods. Once every benefit period. Trifocal Covered at 100%; you pay $0. Up to $45 Once every two benefit periods. Once every benefit period. Polycarbonate Lenses (up to age 19) Covered at 100%; you pay $0. Not Covered Not Covered Once every benefit period. Tint Covered at 100%; you pay $0. Not Covered Once every two benefit periods. Once every benefit period. UV Coating Covered at 100%; you pay $0. Not Covered Once every two benefit periods. Once every benefit period. Scratch Coating Covered at 100%; you pay $0. Not Covered Once every two benefit periods. Once every benefit period. Standard Progressive (Tier 1) Covered at 100%; you pay $0. Not Covered Once every two benefit periods. Once every benefit period. Frames- Frame reimbursement is based on retail value. Any remainder above the Member’s frame allowance is to be charged to the Member, minus a 20% discount, and can be collected at the time of service when a Participating Vision Provider is used. Discount does not apply at Retail Locations for certain proprietary frame brands or when services are received from an Out-of-Network vision provider Frames $100 Up to $40 Once every two benefit periods. Once every two benefit periods. Contact Lenses (in lieu of eyeglasses)— Contact lens reimbursement is based on retail value. The following discounts apply when a Participating Vision Provider is used for any balance exceeding the plan allowance: 15% for conventional; 10% for disposable. Contact lens fitting and follow-up reimbursement is separate from contact lens materials. Discount may not apply at Retail Locations or Contact Fill ®. Standard / Extended Contact Lens Fitting and Follow Up Covered at 100%; you pay $0. Daily wear - Up to $20 Extended wear - Up to $30 Once every two benefit periods. Once every benefit period. Specialty Contact Lens Fitting and Follow Up4 $50 Up to $50 Once every two benefit periods. Once every benefit period.
 UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 2
UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 2