
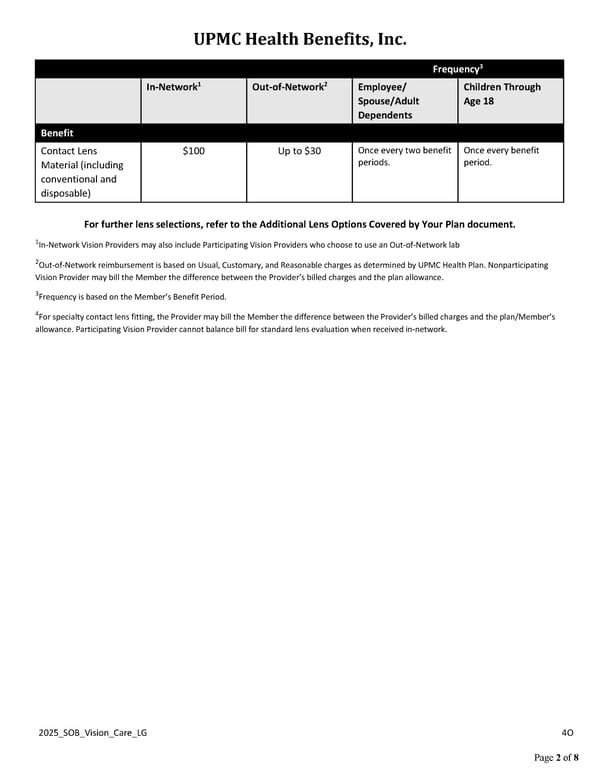
UPMC Health Benefits, Inc. 2025_SOB_Vision_Care_LG 4O Page 2 of 8 Frequency3 In-Network1 Out-of-Network2 Employee/ Spouse/Adult Dependents Children Through Age 18 Benefit Contact Lens Material (including conventional and disposable) $100 Up to $30 Once every two benefit periods. Once every benefit period. For further lens selections, refer to the Additional Lens Options Covered by Your Plan document. 1In-Network Vision Providers may also include Participating Vision Providers who choose to use an Out-of-Network lab 2Out-of-Network reimbursement is based on Usual, Customary, and Reasonable charges as determined by UPMC Health Plan. Nonparticipating Vision Provider may bill the Member the difference between the Provider’s billed charges and the plan allowance. 3Frequency is based on the Member’s Benefit Period. 4For specialty contact lens fitting, the Provider may bill the Member the difference between the Provider’s billed charges and the plan/Member’s allowance. Participating Vision Provider cannot balance bill for standard lens evaluation when received in-network.
 UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 1 Page 3
UPMC Health Benefits: Deluxe Plus Vision Coverage Summary Page 1 Page 3