
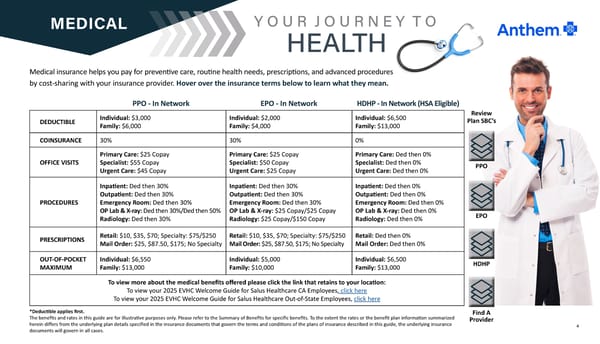
4 MEDICAL Medical insurance helps you pay for preventive care, routine health needs, prescriptions, and advanced procedures by cost-sharing with your insurance provider. Hover over the insurance terms below to learn what they mean. Y O U R J O U R N E Y T O HEALTH DEDUCTIBLE Individual: $3,000 Family: $6,000 Individual: $2,000 Family: $4,000 Individual: $6,500 Family: $13,000 COINSURANCE 30% 30% 0% OFFICE VISITS Primary Care: $25 Copay Specialist: $55 Copay Urgent Care: $45 Copay Primary Care: $25 Copay Specialist: $50 Copay Urgent Care: $25 Copay Primary Care: Ded then 0% Specialist: Ded then 0% Urgent Care: Ded then 0% PROCEDURES Inpatient: Ded then 30% Outpatient: Ded then 30% Emergency Room: Ded then 30% OP Lab & X-ray: Ded then 30%/Ded then 50% Radiology: Ded then 30% Inpatient: Ded then 30% Outpatient: Ded then 30% Emergency Room: Ded then 30% OP Lab & X-ray: $25 Copay/$25 Copay Radiology: $25 Copay/$150 Copay Inpatient: Ded then 0% Outpatient: Ded then 0% Emergency Room: Ded then 0% OP Lab & X-ray: Ded then 0% Radiology: Ded then 0% PRESCRIPTIONS Retail: $10, $35, $70; Specialty: $75/$250 Mail Order: $25, $87.50, $175; No Specialty Retail: $10, $35, $70; Specialty: $75/$250 Mail Order: $25, $87.50, $175; No Specialty Retail: Ded then 0% Mail Order: Ded then 0% OUT-OF-POCKET MAXIMUM Individual: $6,550 Family: $13,000 Individual: $5,000 Family: $10,000 Individual: $6,500 Family: $13,000 To view more about the medical benefits offered please click the link that retains to your location: To view your 2025 EVHC Welcome Guide for Salus Healthcare CA Employees, click here To view your 2025 EVHC Welcome Guide for Salus Healthcare Out-of-State Employees, click here PPO - In Network *Deductible applies first. The benefits and rates in this guide are for illustrative purposes only. Please refer to the Summary of Benefits for specific benefits. To the extent the rates or the benefit plan information summarized herein differs from the underlying plan details specified in the insurance documents that govern the terms and conditions of the plans of insurance described in this guide, the underlying insurance documents will govern in all cases. Review Plan SBC’s PPO EPO - In Network HDHP - In Network (HSA Eligible) EPO HDHP Find A Provider
 SALUS 2025 Benefits Guide Page 3 Page 5
SALUS 2025 Benefits Guide Page 3 Page 5